Sustainable Population Australia (SPA) believes there is nothing to fear from the downward projection of population size in the Inter-Generational Report (IGR) from 40 million to 38.8 million by 2061. National President Jenny Goldie says what is to be feared are the environmental, social and economic cost of adding another 13 million people to the population.
“The IGR fails to take into account the costs of infrastructure which amounts to at least $100,000 in public money for each new person, be they immigrant or born here,” says Ms Goldie.
“The IGR fails to take into account the environmental costs of urban encroachment on natural bushland, threatening iconic species such as the koala, and adding to carbon emissions,” she says. “It fails to address the social costs of crowding, housing unaffordability and longer waiting times that generally accompany population growth.
“Having more people generally means a bigger GDP but not necessarily GDP per capita, which is a better measure of living standards. In fact, GDP is well past its use-by date and, before the end of the IGR time frame, will have ceased to be used. In looking so far into the future, we should be using a range of the newer measures of living standards and well-being.”
Ms Goldie says neither should we fear an ageing population.
“The projection that there will only be 2.7 workers per person aged over 65 in 40 years’ time will probably be wrong,” says Ms Goldie. “In fact, as the working age population shrinks and the labour market tightens, fewer people will be unemployed, and employers will improve wages and conditions to attract job-seekers.
“This will have the effect of drawing more people into the workforce who were not working, or keeping people in work who would otherwise have retired. In other words, the participation rate will improve.”
Ms Goldie says rising health expenditure, while a problem in narrow fiscal terms, is actually a good thing, by keeping people happier and healthier for longer, and by reducing human suffering.
Canadians for a Sustainable Society is a research and activist NGO focused on changing our society’s pursuit of endless growth and ever higher levels of consumption. Simple growth is neither sustainable nor conducive to reducing inequality, debt, fiscal imbalance or achieving environmental sustainability.
Aging is a natural trend towards an increase in the proportion of older people in our population and will continue until the Canadian population stabilizes.
The aging trend is merely part of the much larger demographic transition which has accompanied the development of our modern societies. In this transition, life expectancy has increased from under 40 years in the 1700s to nearly 80 and the number of children per woman has decreased from 6 to near 2.
This demographic transition features:
• lower fertility rates
• longer life spans and
• higher proportions of seniors
Growth Doesn't Pay For It
Aging is inevitable and simply cannot be reversed except by catastrophic population collapse or exponential population growth continuing forever. Aging cannot be supported endlessly by fiscal deficits with the expectation that “growth will pay for it”. Growth does not pay for past deficits as a larger version of a debt producing fiscal structure adds on even larger debts going forward.
Immigration Can't Fix It
Very high levels of immigration has been touted as a “fix” for an aging population. The objective of this fix seems to be to maintain forever the age structure and the rate of growth of the baby boom period. Ie make it the 1950s forever. Attempting to boost immigration to levels which will run ahead of the aging trend will see extreme and ever-increasing levels of immigration with little effect on the age structure.
Why?
The age structure of our immigration stream is not different enough to "youthenize" our population
Aging is a global phenomenon
We Need a Better Strategy
Understanding the nature of the changes and modifying our expectations of endless growth are the challenges which all countries will have to meet. Canada is fortunate in that many advanced societies are decades ahead in this transition and are providing an excellent reference for the development of policies which will allow us to deal successfully with the transition to demographic stability.
The best means of dealing with a shift to a higher proportion of seniors is to boost job quality and flexibility along with wage rates. People must be encouraged to be healthy and the concept of working well past the age previously thought of as “retirement age” must be embraced.
Neither Business-as-Usual nor Business-as-it-Once-Was is sustainable. Make sure your media sources and your political representatives are clear on the need for well-informed progressive change in Canadian public policy. “More of the same” is not a viable strategy.
Canadians for a Sustainable Society is a research and activist NGO focused on changing our society’s pursuit of endless growth and ever higher levels of consumption. Simple growth is neither sustainable nor conducive to reducing inequality, debt, fiscal imbalance or achieving environmental sustainability.
Our group believes that only a comprehensive strategy with relevant national metrics and clear goals can deliver long term social stability and environmental balance.
Jason Kenney in his Backgrounder for his immigration hearing in 2011
“That being said, research underscores that immigration is not a viable remedy for population aging. A 2009 study by the C.D. Howe Institute concludes that improbably huge increases in immigration (i.e. from the current 0.8% to nearly 4% ** of the population) in the short term would be required to stabilize Canada’s current old-age dependency ratio.”
Backgrounder - Stakeholder Consultations on Immigration Levels and Mix
Library of Parliament - Immigration to Canada pdf PRB0350-e - Page 9
“Finally it is worth noting that in 2000, the UN Population Division conducted a study of whether replacement migration could solve the problem of population aging and decline. Using a scenario that simulates the migration required to maintain the dependency ratio the study concluded that the level of immigration to offset population aging would have to be much higher than in the past. For example the United States would have to admit 592 million immigrants between 2000 and 2050 to keep its dependency steady. The population of the United States was 274 million in 2000. This would mean nearly 11 million immigrants each year, compared with 1.5 million at present – not a very realistic scenario”
**The Math: 4% = 1.5 million per
year or 7 new City of Torontos every 10 years,
Compound growth – doubling every 17 years for a population of 36 billion in 2170
Video and transcript inside: Dr Karen Hitchcock: "My core message is that we really need to think about our ageing population as a triumph and really rethink what it means to be old and what it's possible to do when you're elderly. Most elderly people are not sick, most of them are not in nursing homes, but I think we can do a lot more to integrate elderly people back into our communities and try and reimagine what it is that we want our communities to be. I think we need to start from an ethical perspective of what we want our community to be, and then from that, imagine our society and then find ways to create it and fund it, rather than starting from an economic position." Congratulations to the 7.30 Report, Karen Hitchcock and Quarterly essay for criticising the appalling depiction and treatment of Australia's elderly, implicitly and explicitly advocated by the growth lobby in the mainstream media and government. See, for instance, "Should Jeannie Pratt and Elisabeth Murdoch downsize to high rises in Activity Centers to give young people more room?" The negative message about the elderly has been so overwhelming that most of us find it exhausting to fight. The ABC has often also carried this message uncritically. Perhaps it took a woman-led news commentary program - the 7.30 Report - to try to break this mould. Dr Karen Hitchcock (who is a staff physician in acute and general medicine at a large city public hospital) is a very effective ambassador for the elderly, although she is a young woman herself. Her work deserves our collective support and promotion.
Discussion on our ageing population and their use of the healthcare system is sending older Australians a message that they're a burden to society, suggests a physician at a major public hospital in Victoria, Karen Hitchcock.
Transcript
LEIGH SALES, PRESENTER: By 2050, about five per cent of Australia's population will be over the age of 85, with many of us expected to live to our mid-90s. The challenges of the ageing population are something we've been hearing a lot about in the past couple of weeks, since the Federal Government released its Intergenerational Report. The message is that more old people and falling budget revenues are going to put a huge strain on our health and welfare systems. But now one doctor is raising concerns about the way we're discussing the ageing population. She believes we're sending older Australians a message that they're an intolerable burden.
Karen Hitchcock is a staff physician in acute and general medicine at a major public hospital in Victoria and she's written the latest issue of the Quarterly Essay. It's entitled Dear Life: On Caring for the Elderly, she joined me from our Melbourne studio.
Karen, we've been talking a lot recently about the economics of health care as the country deals with an ageing population and declining budget revenue. When you listen to economists and politicians talk about the ageing population and the growing pressures on the budget and sustainability and so on, as a doctor, what do you hear?
KAREN HITCHCOCK, PUBLIC HOSPITAL PHYSICIAN & AUTHOR: What I hear is that the fact of our ageing population is an overwhelmingly negative development. The elderly are portrayed as being a burden on their families and on the state and a drain on the economy.
LEIGH SALES: And what message do you think that the elderly hear?
KAREN HITCHCOCK: Oh, I think that they've completely internalised this message that they're a burden. I see evidence of this every day on my hospital ward. Patients, elderly patients apologise for being sick, for being in hospital, for taking up a hospital bed that should be apparently for somebody else.
LEIGH SALES: How does that translate then in terms of the type of care that they want?
KAREN HITCHCOCK: Well, I think that sometimes it can mean that they feel reluctant to accept the care that they need.
LEIGH SALES: Like, give me an example of, say, a patient where you've seen that.
KAREN HITCHCOCK: Um, well, I've - there's a lot of patients, but recently I looked after an elderly gentleman who said that he wanted to die and that he didn't want to be in hospital and that he was a nuisance and when I sat down and talked to him, it turned out that his wife had recently died, his dog that was his remaining companion had died and he felt that he had no place in society anymore and that he was a burden.
LEIGH SALES: And so how, as a doctor, did you address that?
KAREN HITCHCOCK: I called him a couple of weeks after he left hospital, given that he had said he never wanted to come back to hospital, just to try and work out a plan for him and he said to me that he says silly things when he's sick. Of course he wants to come back to hospital and that he was very, very happy because he'd managed to get another dog, go back to his part-time work.
LEIGH SALES: What's your attitude towards advanced care directive, which are documents that people sign giving instructions about the sort of treatment that they would like if they're faced with potential end-of-life issues, which of course is often things that older people sign?
KAREN HITCHCOCK: They're being heavily promoted at the moment as something that should be universally adopted and I think that they do have a place, particularly if people have advanced malignancy and are going to die imminently or particularly when people have particular treatments that they don't want to have. But I think that saying that every single citizen in Australia should have an advanced care directive is dangerous and I think that to say that they're unambiguously good sort of relies upon an understanding of the human subject that is breathtakingly simplistic. People change their mind. It's very difficult for us to know how we're going to feel as we become increasingly dependent and debilitated. I mean, my grandmother, for example, she was a fiercely independent woman who, in her 80s, developed a lung disease that meant eventually she was house-bound and oxygen dependent. And if someone had've asked her a year prior to that development whether or not she would rather die or be house-bound and oxygen dependent, she definitely would have said she'd rather be dead. But when it came down to it, she was very happy with her life. She still had her family. She said that she would play in her memories. She was very happy to be alive.
LEIGH SALES: So if you see this idea that we are giving elderly people the impression that they're a burden as being a problem, how would you like to see the debate around some of these issues and the discussion reframed?
KAREN HITCHCOCK: Well I think that our focus should be on how can we improve the life of our elderly patients, not that we should be so keen to offer them death.
LEIGH SALES: And so, practically, how would you go about doing that?
KAREN HITCHCOCK: Um, I think that we - it would be really helpful if we could somehow integrate medical and social services so that we can encourage elderly people to remain independent and in their communities. If we could somehow integrate services and offer preventative treatment before people need to come to hospital, that would be a really great development and there are international examples of care programs like this where there are community-based, what's called medical homes, that are staffed by GPs and specialists and full allied health to enable people to stay in the community longer and to stay well and independent.
LEIGH SALES: How about the interaction between nursing homes and hospitals, how well does that work?
KAREN HITCHCOCK: It works very poorly. Many elderly people come to hospital as a result of medication side-effects, having too many tablets or etc., and they come to hospital, we stop their tablets and they're discharged back to their nursing homes and they have to continue on the tablets that they were on prior to coming to hospital, sometimes the tablets that caused them to come to hospital, until they can get a doctor to come to the nursing home and rechart their medicine.
LEIGH SALES: You are a busy doctor, yet you've taken the time out to write this lengthy piece of work around these issues. What is the core message that you're hoping to get out there based on your experience working in hospitals?
KAREN HITCHCOCK: My core message is that we really need to think about our ageing population as a triumph and really rethink what it means to be old and what it's possible to do when you're elderly. Most elderly people are not sick, most of them are not in nursing homes, but I think we can do a lot more to integrate elderly people back into our communities and try and reimagine what it is that we want our communities to be. I think we need to start from an ethical perspective of what we want our community to be, and then from that, imagine our society and then find ways to create it and fund it, rather than starting from an economic position.
LEIGH SALES: Just before you go, Dr Hitchcock, there's been a lot of discussion around this week about sexism in medicine. A senior surgeon raised some concerns around the issue of sexual harassment and whether or not raising that impacts on female doctors' careers. Just in your experience, do you think that there is a problem in medicine with sexism?
KAREN HITCHCOCK: I've obviously not worked with every doctor in every hospital in Australia and I'm sure there are individuals. However, one thing I do know is that there is certainly not a pervasive culture of sexism in medicine. I've never been discriminated against because I'm a woman in medicine. In fact I've been enormously supported and encouraged.
"Allowing more migration from Asia could help Australia cope with the challenges of its ageing population, a leading economist says," quoth Fairfax Digital. Ditto Murdoch's Australian: "More Asian migration would help Aust: HSBC". The 'leading economist' is Paul Bloxham, who is employed by HSBC Australia bank with the title of 'chief economist and spokesperson'. The publishing media are heavily invested in marketing Australian real estate to the world.
This narrowly-based opinion is published and promoted as 'breaking news' by Australia's mass media as if it were a disinterested and unquestionable truth, but it comes from a person paid by a business corporation to spruik their interests and it is reported by media giants who also have massive interests in property development and finance.
Fairfax media and Murdoch media both have huge property dot coms that market Australian real estate. These are Realestate.com.au and Domain.com.au. Other media organisations also massage the property market with television lifestyle programs etc. The Australian public is utterly manipulated in this area by the media, yet the media continue to promote their own interests without declaring them in articles like the ones quoting Bloxham.
It could be that HSBC Bank really believes that what is good for their global banking business headquartered in London and which started in Asia [1] is good for Australia, but their chief economist shows extremely poor understanding of Australian demographics.
Misleading demographics
Paul Bloxham is actually quoted as saying that,
"Migrants are typically younger than the extant population." (!) To which he adds, "The ageing population means greater spending on healthcare and less revenue from the income tax system, putting strain on government budgets," Mr Bloxham said.
Such a statement assumes that Asian migrants must have the solution to eternal youth, and don't age one year every year like other people. It doesn't acknowledge that all immigrants to Australia are older on entry than those born here, tend to import elderly family (under family reunion terms) and thus to contribute overwhelmingly to a more rapid aging demographic in Australia. This has been shown by the Federation of Ethnic Communities' Councils of Australia (FECCA), who have been campaigning for special aged care funding geared to the higher rate of aging in immigrants. See, "Immigration speeds up Australia's rate of aging - FECCA" :
"From 2011 to 2026 ethnic people over 80 will increase by 59% compared with 29% in the Australian-born population." FECCA.
Even the mysterious Multicultural Foundation of Australia, founded by Bob Hawke in 1986, of which every recent Prime Minister and Opposition leader are members, funds research to deliver education on dementia for the rising proportion of aging immigrants.
And Access Economics, in an August 2009 Report that the AMC and FECCA both rely on, states:
"Of people with dementia in 2009, the majority speak English at home (211,000) compared to a non-English (CALD) language (35,000). The prevalence of people with dementia speaking English at home increases 4.8 times to 1.01 million in 2050, with those speaking a CALD language at home increasing 3.4 times to around 120 ,000 in 2050. The tripling in the absolute number of people with dementia who speak a CALD language at home represents a very significant increase in the future demand for CALD trained dementia care providers and culturally appropriate services. "
Why don't HSBC suggest importing these immigrants to Australia, and sending them home when they retire?
A violation of self-determinism and human rights
Adding more people won't solve an imbalance of ageing people. Migration means ultimately that each generation will have an even bigger ageing population to cater for!
In a comment made todayBandicoot wrote, "HSBC finance mortgages and investment property loans. Migrants will want property loans, and bring in investors. This is propaganda thinly disguised as demographic advice to promote their interests, and expect the public to swallow it, and pay for it!
Surely the people of Australia have had enough of corporate control, and our population growth has been controlled for too long by vested interest groups? Population control, through tweaking of demographic trends for constant growth, is a violation of self-determinism and human rights."
"Headquartered in London, the HSBC Group serves customers worldwide from around 6,300 offices in over 75 countries and territories in Europe, Hong Kong, Rest of Asia-Pacific, North and Latin America, and the Middle East and North Africa. With assets of US$2,671bn at 31 December 2013, the HSBC Group is one of the world's largest banking and financial services organisations. [...]
HSBC's strategic direction reflects its position as 'The world's leading international bank', combining the largest global emerging markets banking business and a uniquely cosmopolitan customer base with an extensive international network and substantial financial strength.
The Group's strategy is aligned with the key trends which are shaping the global economy. In particular, HSBC recognises that, over the long term, developing markets are growing faster than the mature economies, world trade is expanding at a greater rate than gross domestic product and life expectancy is lengthening virtually everywhere.
HSBC's strategy is focused on delivering superior growth and earnings over time by building on the Group's heritage and skills. Its origins in trade in Asia have had a considerable influence over the development of the Group and, as a consequence, HSBC has an established and longstanding presence in many countries. [...]"
Ausfis is one of many private immigration agencies in Australia promoting a problematic political message that sounds like they are representing all Australians and the Australian government and which many Australians would disagree with. Should migration agencies aggressively promote immigration? It's another case of advertising taking over democracy.
Ausfis's talk about 'a new land of opportunity' belies the biogeophysical reality of Australia - the oldest, driest continent.
This is a link that was sent to an immigrant from Peru from someone living in Peru - about inviting migrants to come to Australia because we have opportunities and skills shortages!
It not only refers to skill shortages, but it suggests that its lawyers will get applicants citizenship after four years and encourages immigrants to bring their dependent family members to live here as well, receive health care and use the public education system.
"What are the benefits of receiving a visa via the General Skilled Worker Visa program?
The grass is greener in Australia. If you are planning to make a move outside your home country, Australia should be on the top of your list as a place to make your dreams a reality. Besides legally living and working in Australia, a Australian General Skilled Visa has other benefits,
such as:
Bringing all dependent family members with you
Receiving healthcare
Using the public education system
Applying for citizenship after 4 years!"
Immigration greatly accelerates ageing of Australia's population: FECCA
Note that FECCA has only recently published a paper "Immigration speeds up Australia's rate of aging - FECCA"calling for special funding for aged immigrants because of the way immigration ages the Australian population. Every immigrant comes here older than anyone born here, but this fact is grossly magnified by the effect of bringing dependent adults as extended family here. Between 2011 to 2026 ethnic people over 80 will increase by 59% compared with 29% in the Australian-born population. Continuing high immigration threatens to make this problem unmanagable, with stress on housing, employment, water, food and power supplies undermining democracy, health and life-expectancy.
Ausfis looks very official and could easily be mistaken for an Australian Government website and message, but it isn't. It is a private business composed of people who make money out of processing migration applications. In fact, it does clearly state what it is at the bottom of the page and the agency promotion style seems responsible. It is not doing or saying anything illegal or misleading; it is, indeed, apparently promoting government policy.
Currently immigration to Australia outweighs births over deaths. It is the main source of population growth here.
"Increased migration and fertility (2007–2011)
Source: http://www.abs.gov.au/ausstats/[email protected]/Lookup/2071.0main+features952012-2013
Despite the economic impacts of the global financial crisis which started in 2007 and the ongoing repercussions within global financial markets, Australia experienced strong and sustained population growth throughout the period 2007–2011 (see the graph of Annual population growth above). In 2009, the addition of 394,000 people was the highest single annual increase to Australia's population, and the annual growth rate of 1.8% was unmatched since 1972. Migration was a significant factor in the population growth during this period. For the first time since federation, migration consistently contributed more to population growth than the contribution from natural increase. However, much of this recent increase has come from increased numbers of long-term temporary migrants; those with student, holiday and business visas (for more information see Migration, Australia (cat. no. 3412.0). The effect of this high level of migration can be seen in the 25–29 years age group in 2011, where there were an additional 385,000 people compared with the numbers in this cohort when they were aged 5–9 years in 1991. "
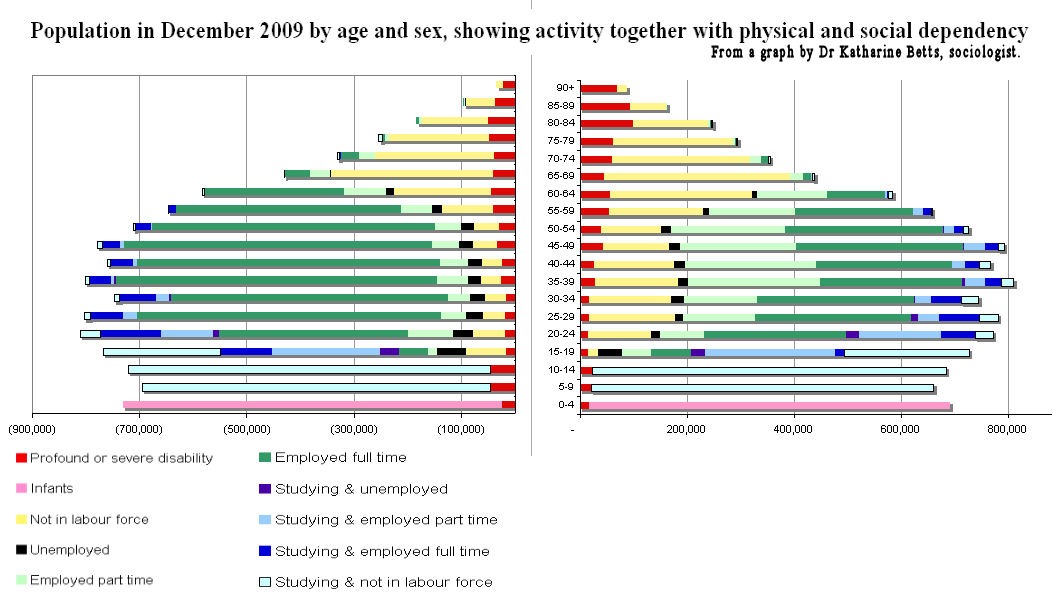
Sources: Disability, Ageing and Carers: Summary of Findings, Australia 2003, Catalogue no. 4430.0, ABS, Canberra, 2004; Labour Force, Australia, Detailed - Electronic Delivery, Catalogue no. 6291.0.55.001; General Social Survey 2006, Confidentialised Unit Record File supplied by the ABS
Notes: The ABS defines a profound disability as one where the person always needs help with one or more of the activities involved in communication, mobility and self care, and a severe disability as one where the person sometimes needs such help.
The data on labour force participation are for December 2009, but detailed age break downs were only available for June 2009. All of the data have been standardised to the age/sex structure of the population in June 2009.
Graph by Assoc. Prof. Dr Katharine Betts, (Swinburne University, Victoria) author of Immigration Ideology, MUP, 1988 and The Great Divide, Duffy and Snellgrove, 1999. She is also the co-editor, with Bob Birrell, of the Monash demographic quarterly, People and Place..
Hyperacusis - a misunderstood source of social friction in a densely packed society
Those who find particular sounds unbearable, but who don't get understanding from their friends and relatives, should find out about the condition of hyperacusis at this hyperacusis site. The website was created through the contributions of clinicians and patients from all over the world, who joined together to establish an extensive source of information to help patients recover from hyperacusis. It was by fully reading this site that I came to some understanding and tolerance of the level of complaint about dogs barking on this forum. The following site has a massive amount of helpful information, including case histories, a self-help treatment option, and specialist referral services. The self-help treatment option (using a cd with 'pink noise') is very low cost (instead of USD $3-4,000) and there are several accounts on-line of how it helped people to easily accomodate common sounds which they previously found intolerable. Even if you are not a sufferer, the syndrome is a very interesting one to read about. In fact all of us, as we grow older, may be at risk of symptoms of the 'recruitment' syndrome described below, although most people will not experience it in a devastating way.
Of particular interest was the page, which gives information about four kinds of hyperacusis, which I reproduce below.
"4 Types of Sound Sensitivity"
"1. HYPERACUSIS: These individuals have a collapsed tolerance to normal environmental sound. The term commonly used to describe this condition is 'hyperacusis'. Hyperacusis can come on gradually or occur suddenly where the patient finds themself in a state of crisis. Patients who have a collapsed tolerance to sound need to have their Loudness Discomfort Levels (LDL's) established by a hearing healthcare professional. Normal LDL's are in the 85-90+ decibel range. Patients with hyperacusis would have LDL's well below that level. The common treatment for hyperacusis is listening to broadband pink noise though sound generators (special hearing aids) which must be ordered through a specially trained doctor or audiologist who administers Hyperacusis (Tinnitus) Retraining Therapy. The therapy often costs $3000-$4000 (depending on the clinician) and typically is not covered by insurance.
There are two basic ways to deliver broadband pink noise to your ears. The best way starts with a clinician who is trained to diagnose the seriousness of your condition, explain to you the dynamics of hyperacusis, test your ears in gentle ways to determine your loudness discomfort levels (LDL), fit you with special hearing aids called noise (sound) generators that deliver broadband pink noise to your ears, monitor your progress and provide directive counseling until you recover. Treatment usually lasts 6 months. Clinicians who administer this kind of treatment were trained by Dr. Pawel Jastreboff (Emory University in Atlanta, Georgia). They are experts in treating hyperacusis and tinnitus patients. Their protocol is called Tinnitus Retraining Therapy (also know as TRT) and it has significantly helped tinnitus and hyperacusis patients recover. To learn more about TRT you might consider reading Dr. Jastreboff's book "Tinnitus Retraining Therapy." A list of TRT clinicians can be seen by visiting this website: http://www.tinnitus-pjj.com/referral.html
The second way one can deliver broadband pink noise to their ears would be to purchase the broadband pink noise CD from the network. Instead of listening to broadband pink noise through special noise generators (TRT), a similar sound can be delivered to the ear by listening to a pink noise CD. With this method pink noise is delivered to the ears through a compact CD player (i.e. walkman). If you use a compact CD player it is very important that you use open air headphones. More detail is explained in the guideline that comes with this networks pink noise CD. Pink noise can also be downloaded from the pink noise CD to an ipod. The only caution here would be that the pink noise be converted to a WAV or AIFF format.
2. RECRUITMENT: There are many more individuals who have recruitment. Recruitment is the a rapid growth of perceived loudness for sounds in the pitch region of a person who has hearing loss. This phenomenon occurs because at some decibel level, the normal hair cells adjacent to the damaged hair cells (corresponding to the frequency of a hearing loss) are "recruited." At the decibel level at which these normal hair cells "kick in," perceived loudness shoots up rapidly, causing discomfort. In other words, at one point the person cannot hear the sound because they have hearing loss (in that frequency), then when the sound reaches a certain loudness and/or frequency the person is blown away. Once they finally hear the sound, it is perceived as far too loud. Recruitment is a common phenomenon in cultures where the majority of their lives have been saturated with too much noise – like our Western culture. Common treatment is the same as it is for hyperacusis unless the persons hearing loss is so pronounced that listening to broadband pink noise would be of no benefit to them.
3. HYPERACUTE HEARING: Then there are individuals who are sound sensitive at birth but it is only specific to certain frequencies heard at loud levels (typically above 70 decibels). It may seem like we are splitting hairs here but remember – the key words with hyperacute hearing are – sound sensitive to specific frequencies heard at loud levels. These frequencies are typically labeled 'problem' frequencies. Autistic children are good examples of this. They can tolerate some sound at normal or even loud volumes but some frequencies are intolerable. Commonly autistic children, children who are marginally autistic, or non-autistic individuals who have hyperacute hearing are treated with auditory integration therapy (AIT). AIT takes regular music and filters out the problem frequencies through a special machine called an audiokinetron. Somehow this therapy seems to 'retune' their ears and normalizes their hearing tolerances. The music is listened to at decibel levels which can peak up to 90 decibels. This creates a problem for the hyperacusis patient. The therapy is too loud and only worsens the condition of the hyperacusis patient whose Loudness Discomfort Levels have been compromised. Hyperacusis and recruitment share part of a common pathway but in some ways we are very different and our retraining therapies run very much a different path.
Phonophobia often develops with an individual who has a significant collapsed tolerance to sound. They not only fear the sound of the environment they are experiencing in real time (right now) they worry about the sound that future events of the day or in the near future will produce. Phonophobia can take over ones life and make one feel they need to isolate themselves to survive. This is a recipe for disaster. It is critical that we keep our ears active to rebuild our tolerances to sound. That is why broadband pink noise is so crucial to bringing us back to the mainstream of life.
4. MISOPHONIA: (dislike of sound) has often been thought to be hyperacusis. This is not true. Let us be clear here. A hyperacusis patient can have a strong fear of sound (phonophobia) or a specific dislike of specific soft sounds (misophonia) but neither one of these symptoms stand alone as hyperacusis.
Hyperacusis is a collapsed tolerance to normal environmental sounds. They hyperacusis patient may or may not have phonophobia and/or misophonia. If the hyperacusis patient IS also dealing with phonophonia and/or misophonia then their clinician needs to address these issues is addition to treating the patient for hyperacusis. It is also important to note that a person can have phonophobia and/or misophonia and not have hyperacusis at all. Sound confusing. Let's talk...
We will discuss forms of misophonia. They are not a separate catagory of sound sensitivity because the issues we are about to talk do not involve loud sounds. Some individuals are not sensitive to loud sounds (in other words they have normal loudness discomfort levels - LDL's) but they are unable to tolerate the sound of people eating or chewing. Oddly enough they have no problem tolerating the sound of their own eating. These individuals have a difficult time eating with their family and friends and some insist on eating all by themselves. They become irritated or enraged at meals and sometimes. This is not hyperacusis. The patients primary goal would be to neutralize or refocus the dislike they have of these specific sounds. Most of these individuals live very normal lives with the only exception of being unable to tolerate all the dynamics of other people eating. Often these individuals have been unsuccessful finding any information about this condition. To the best of our knowledge no articles have been written in any qualified medical journal and no studies or research has been done about this. Patients seeking treatment from their clinician may have to copy the information from this website to help their doctor understand what is taking place here. Treatment for these patients comes from clinicians who have a specific protocol for misophonia. Search the network message board using the word 'misophonia' to learn more about this problem and protocols suggested. Usually these individuals are sensitive to particular sounds which are not loud in volume. For example, some individuals have a hearing sensitivity to certain consonants (i.e. s, t, p, c). Once again, although this is a sound sensitivity issue, this is not hyperacusis. It is misophonia.
Misophonia is a symptom which is misunderstood. The word 'misophonia' was invented by Dr. Pawel Jastreboff to help clear some of the misunderstanding. Aside from a misophonia protocol it is not clear whether broadband pink noise helps the patient improve their dislike of sound. Some individuals with misophonia have been diagnosed with an obsessive compulsive disorder (OCD) and have sought treatment from a psychotherapist."
 Sustainable Population Australia (SPA) believes there is nothing to fear from the downward projection of population size in the Inter-Generational Report (IGR) from 40 million to 38.8 million by 2061. National President Jenny Goldie says what is to be feared are the environmental, social and economic cost of adding another 13 million people to the population.
Sustainable Population Australia (SPA) believes there is nothing to fear from the downward projection of population size in the Inter-Generational Report (IGR) from 40 million to 38.8 million by 2061. National President Jenny Goldie says what is to be feared are the environmental, social and economic cost of adding another 13 million people to the population.



 Video and transcript inside: Dr Karen Hitchcock: "My core message is that we really need to think about our ageing population as a triumph and really rethink what it means to be old and what it's possible to do when you're elderly. Most elderly people are not sick, most of them are not in nursing homes, but I think we can do a lot more to integrate elderly people back into our communities and try and reimagine what it is that we want our communities to be. I think we need to start from an ethical perspective of what we want our community to be, and then from that, imagine our society and then find ways to create it and fund it, rather than starting from an economic position." Congratulations to the 7.30 Report, Karen Hitchcock and Quarterly essay for criticising the appalling depiction and treatment of Australia's elderly, implicitly and explicitly advocated by the growth lobby in the mainstream media and government. See, for instance,
Video and transcript inside: Dr Karen Hitchcock: "My core message is that we really need to think about our ageing population as a triumph and really rethink what it means to be old and what it's possible to do when you're elderly. Most elderly people are not sick, most of them are not in nursing homes, but I think we can do a lot more to integrate elderly people back into our communities and try and reimagine what it is that we want our communities to be. I think we need to start from an ethical perspective of what we want our community to be, and then from that, imagine our society and then find ways to create it and fund it, rather than starting from an economic position." Congratulations to the 7.30 Report, Karen Hitchcock and Quarterly essay for criticising the appalling depiction and treatment of Australia's elderly, implicitly and explicitly advocated by the growth lobby in the mainstream media and government. See, for instance,  "Allowing more migration from Asia could help Australia cope with the challenges of its ageing population, a leading economist says," quoth
"Allowing more migration from Asia could help Australia cope with the challenges of its ageing population, a leading economist says," quoth  This narrowly-based opinion is published and promoted as 'breaking news' by Australia's mass media as if it were a disinterested and unquestionable truth, but it comes from a person paid by a business corporation to spruik their interests and it is reported by media giants who also have massive interests in property development and finance.
This narrowly-based opinion is published and promoted as 'breaking news' by Australia's mass media as if it were a disinterested and unquestionable truth, but it comes from a person paid by a business corporation to spruik their interests and it is reported by media giants who also have massive interests in property development and finance. 

 Ausfis is one of many private immigration agencies in Australia promoting a problematic political message that sounds like they are representing all Australians and the Australian government and which many Australians would disagree with. Should migration agencies aggressively promote immigration? It's another case of advertising taking over democracy.
Ausfis is one of many private immigration agencies in Australia promoting a problematic political message that sounds like they are representing all Australians and the Australian government and which many Australians would disagree with. Should migration agencies aggressively promote immigration? It's another case of advertising taking over democracy. Ausfis's talk about 'a new land of opportunity' belies the biogeophysical reality of Australia - the oldest, driest continent.
Ausfis's talk about 'a new land of opportunity' belies the biogeophysical reality of Australia - the oldest, driest continent.
Recent comments