RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come.
The Royal Australian College of General Practitioners (RACGP) is warning government that GPs will need adequate resources to manage the long-term care of COVID-19 positive patients. The RACGP has released a guide for GPs providing care to adult patients who have previously tested positive to COVID-19 or have a history suggestive of undiagnosed COVID-19 and have - or are at risk of - post-COVID-19 conditions. The guide was developed in collaboration with HealthPathways. RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come.
“Some COVID-19 positive patients quickly make a full recovery but that is certainly not the case for all people,” he said.
“Evidence is emerging that some patients are being left with serious physical, cognitive and psychological impairments that will require long-term care. For these patients, it is not a case of contracting the virus, getting better and never thinking about it again.
“Post-COVID-19 conditions include lung scarring, post-viral fatigue as well as ‘brain fog’. Emerging data suggests that up to 80% of people with severe cases of COVID-19 resulting in hospitalisation will experience post-COVOD-19 conditions.
“There is also evidence that people who have contracted COVID-19 exhibit neurological symptoms, from loss of smell, to cognitive impairment, to an increased risk of stroke. There are also potential long-lasting consequences such as post-traumatic stress disorder (PTSD) following severe illness, liver dysfunction, and heart failure.
“These long-term effects are likely to be particularly severe for older people, those with chronic disease and those who experienced severe acute COVID-19. GPs will be crucial in managing the health and wellbeing of these patients in the years ahead.”
The Acting RACGP President said that GPs need government support in caring for the potentially significant needs of patients with post-COVD-19 conditions.
“When we look at the patients most likely to suffer severe post-COVID-19 health concerns it is older people and those with multiple chronic conditions, including patients who have delayed or avoided care during the pandemic,” he said.
“A voluntary patient enrolment model, where clinics receive additional payments for ‘enrolling’ a patient with a regular GP, would be particularly beneficial for these patients. This model enhances comprehensive care for patients and reduces hospitalisations for those who frequently visit GPs.
“Post-COVID-19 health impacts will take a significant toll on many patients including on their mental health. The guide is mindful of this and includes information on accessing mental health services or online supports.
“The Federal Budget included a $100.8 million investment in extending the doubling of Medicare-subsidised psychological therapy sessions for people who have used their initial 10 sessions.
“That is a welcome announcement that will make a real difference. However, in the longer term, many patients including those suffering the after effects of COVID-19 would benefit enormously from new Medicare subsidies for longer consultations.
“Longer consultations allow GPs to take the time to talk through what our patients are experiencing and how we can help them.
“Similarly, new Medicare subsidies for longer consultations for people with chronic conditions would be very helpful. These are the patients who require a bit more time and attention, particularly if they have had COVID-19.”
The guide includes information on:
· infection control precautions and advising patients that having COVID-19 may not confer complete immunity
· collaborating with the patient to develop an individualised plan to support their recovery. This also presents a unique opportunity to optimise the management of existing chronic conditions
· providing care for specific groups recovering from the virus including those with severe COVID-19 requiring hospitalisation, older patients and people with disability
· options for enhancing support for patients including home delivery of medicines, assistance with food and meals and support lines including the Older Persons COVID-19 support line.
"Can the people with COVID suffer long term effects? Including long term effects that affect the brain? Yes. These are the so-called “long-haulers.” And it is not necessarily just people with COVID who have required the intensive care unit."
"Dexamethasone, a steroid medication, specifically a glucocorticoid. Yes, it can cause anxiety, irritation, psychosis, delirium, sleep disturbance. This is why when we do give steroids, we try to avoid giving them before sleep. When assessing someone’s mental status, or psychiatric state, its important to know what they are normally like at their baseline. Are they acting differently? That’s really what you’re looking for. Steroids are prescribed very frequently, and these side effects, are not necessarily rare, its not like we give steroids and necessarily expect them to have these side effects. It's very hard to put a number on how often these side effects occur because there are so many different medications that can cause these symptoms and so many other factors that can contribute towards mental status changes. So you will never get a concrete number on how often these mental side effects occur, but if I had to put a number, I would say less than 10%, at least based on my experience of giving thousands of patients steroids.
Well, let me start out by saying there are over 30 million documented COVID cases and 1 million deaths worldwide, and over 200,000 deaths in the US. The clinical spectrum of disease can range anywhere form no symptoms to mild symptoms, to pneumonia, to ARDS and shock with multiorgan failure, and death. Because COVID is a new disease, the possible long-term health consequences, are still not well-known. So these long-term effects of COVID, we can call this postacute COVID, defined as the presence of symptoms extending beyond 3 weeks from the initial onset of symptoms. And Chronic COVID is beyond 12 weeks.
But postacute COVID syndrome is not just seen in those who had a severe illness and were hospitalized. In a telephone survey conducted by the CDC among a random sample of 292 adults (≥18 years) who had a positive outpatient COVID test and were symptomatic, 35% said they did not return to their usual state of health 2 weeks or more after testing. And this occurred in all ages of adults.
The most commonly reported symptoms after acute COVID are fatigue and dyspnea. And this is exactly what I’ve been seeing with some of my patients with COVID. This persistence of fatigue, and feeling short of breath. Other symptoms include joint pain and chest pain. In addition to these symptoms, there are cases of patients with specific organ dysfunction, primarily involving the heart, lungs, and brain. This might be a result of the viral invasion, by hijacking those ACE2 receptors in our body, but it can also be related to the intense inflammation and cytokine storm, or a combination of these.
In a study of 55 patients with COVID, at 3 months after discharge, 35 had persistent symptoms and 39 had abnormal findings on chest x-ray or CT scan, meaning interstitial thickening and evidence of fibrosis, meaning scarring. In 2 different studies that were done, they looked at patients with COVID who were discharged from the hospital. At about three months after discharge, about 25-30% of patients had at least some impairment in lung function, as evidenced by pulmonary function tests.
Heart damage, aka myocardial injury, as defined by an increased troponin level in the blood, has been described in patients with severe acute COVID. Inflammation of the heart muscle, meaning myocarditis, in addition to heart arrhythmias, has also been described after SARS-CoV-2 infection. I dedicated an entire video to this topic, so you can check that out for more details. The virus that causes COVID, SARS-CoV-2, can infiltrate brain tissue when the virus gets in the blood. It can also get to the brain by invading the olfactory nerve, which is the nerve responsible for the smell. This is why the loss of smell is a common symptom. Besides the loss of smell and loss of taste, the most common long-term neurologic symptoms after COVID are headache and dizziness. Less common, but still possible, is stroke, brain inflammation, meaning encephalitis, and seizures. In previous pandemics with SARS, MERS, and influenza, some people who recovered from those illnesses had neuropsychiatric issues that lingered for months. So were talking about cognitive health here, like depression and anxiety. And the post-COVID is known to cause “brain fog” and mood swings, this has been reported up to 2 to 3 months after initial COVID" illness. [Source: Partial transcript accompanying the video above.]
[English translation of video-dialogue below the video.] In this very interesting video, Frederic Taddei of Interdit d'interdire (Forbidden to censure) states, at the beginning, that he has no intention of evaluating the value of hydroxycloroquine and azithromycine, because he lacks the medical knowledge to do so. He states his intention in inviting his guests (Olivier Berruyer, economist and statistician, and Raphaël Liogier, sociologist and philosopher) is to find out why there is so much controversy over Professor Didier Raoult and his promotion of COVID-19 treatment using hydroxychloroquine. [Note that this unpolished translation took hours out of several days. Both debaters spoke emotionally and with multiple redundancies, also different versions of the word hydroxychloroquine.] Among other things, the participants' discussion of the politics seemed to boil down to the ambiguity of testing drugs in a pandemic situation where big-pharma, other commercial competition, and fraud, loom. I thought that the main argument could be summarized as: (Olivier Berruyer) 'The effectiveness claimed by Didier Raoult for hydroxychloroquine could only be proven through randomised double-blind trials, but these have never been successfully completed due to a series of mishaps', and 'There is no way anyone could scientifically reproduce Raoult's method because he keeps changing it', versus (Raphael Liogier) 'Pending a perfect cure for COVID-19, Didier Raoult is doing the best he can as he treats people in a personalised manner, monitoring their responses, with drugs he believes to be effective'. I would add that, as the translator, and as an evolutionary sociologist, my own feeling about the reasons for such controversy is that it is related to the way apes behave over a tasty food supply or some other big event (good or bad) that concerns them. It is natural for everyone in the community to get involved in something important - in this case a pandemic. We seize whatever handle, whatever fact or factoid we can get hold of, and we run with it, to the best of our ability and enthusiasm. Apes with alpha-pretensions get up in trees and shout loudly about what they've got, competing for audiences and power. So, I invite the reader to keep in mind ape-ethology when he/she reads the translated dialogue below. {See also the notes at the end, on hyrdoxychloroquine trials and prescription of this drug and the law in France.)
FREDERIC TADDEI (Host of Interdit d'Interdire): But the controversy around Professor Raoult goes beyond all that. For four months the lines have been drawn between those who believe in Raoult and those who don't believe in him. It has become a real war of religion. So, although we cannot debate the existence of god, or faith, or miracles - you either believe in them or you don't - we can debate the sacred literature. That's what we are going to do, with a pro- and an anti-Raoult, since France has been divided into pro- and anti-Raoult. My two guests are not medical doctors, but they have looked into what Didier Raoult says. The first guest is Raphael Liogier. He is a philosopher and sociologist, professor at the institute of political studies in Aix en Provence.
FREDERIC TADDEI [Addressing Liogier]: You are the author of Sacred medicine, history and future of a sanctuary of thinking, with Jean Bauberot, and of the Horror of emptiness, a critique of industrialist thinking, which will come out at the beginning of the school year, [...] and which will talk about, notably, the politics surrounding Didier Raoult. I will add that you are a member of the ethics committee at Didier Raoult's Marseille IHU [IHU = Instituts Hospitalo-Universitaires], and that you took part in the editing of the report at the request of Professor Raoult, on how to articulate research and care, in a time of pandemic. This report is expected to be available soon, and everyone will rush to read it. So, for you, who defend the work of Professor Raoult, what is the meaning of all this controversy, in two words, RapHael Liogier?
Interdit d'interdire - L'affaire Didier Raoult
RAPHAEL LIOGIER: Over and above, the polemics, it's much deeper. We are looking at a loss of credibility in science and a transformation of the major scientific paradigms. Whilst we are talking about things like randomised double blind trials, we are talking about a method that is supposed to be able to find a pure and absolute drug. Then, on the other side, we have Didier Raoult's methodology which is, in fact, a methodology more of feeling one's way; it's more relativist: one seeks, one looks at what works and what does not work. There isn't that background, paradoxically, that is almost religious, in fact, where the religious are not on the side you would expect. They are more given over to positivism and rationalism. The philosopher, Hegel, said that everything real is rational. My feeling is that the anti-Raoults are like Hegeliens who defend a kind of industrialist ideal of controls, research, truth, perfect drug, etc. This whilst, in a way, society has largely gone past that. And that's the quarrel, the meaning of the quarrel, in the most profound meaning of the term. I think that's it. We are looking at two different conceptual approaches, two different scientific paradigms, clashing.
Now we go to Olivier Berruyer, founder of the Les-Crises site which specialises in deconstructing propaganda; Olivier Berruyer, who wrote a study that was very critical of Didier Raoult's work, based on Raoult's publications and his assertions. For you, Olivier, what underlies this controversy?
OLIVIER BERRUYER: I would not put myself in an anti-Raoult camp. Raoult was one of the only ones to do a very interesting piece of work on sequelae, scanning infected people [...], so I'm not anti-Raoult, in fact. I am pro-the fundamental principles of science; that's true. I would say that underlying this controversy is that we are becoming a conflict-oriented society. Everyone tries to get a position against something, much more than they do to be for something. This is really quite interesting. The major media push for this, in order to create some buzz, clicks, to sell more paper, but, in the end, one notices that this pushes people to not use their critical faculties to try to find the truth, or at least to come together to create situations where they can discuss it together, but can cause a fairly large number of people to become fanatical, using their critical faculties to confirm their biases, rather than doubting - and science is made up of doubting, and Russell said, "Never be certain of anything." In any case, have reasonable doubts, don't over-doubt, because that will also prevent you from reaching the truth. For me, it's really that: this story of strange passions, when instead one could discuss the subject peacefully. I do hope we will enter reality and leave this sort of Orwellian truth potion, where each person invents their own reality. When we live in different realities, we can no longer communicate.
FREDERIC TADDEI: Let's start then by what you don't like, Olivier, in Professor Raoult's work, since you have said that you are not an 'anti-Raoul', and that you admire him for a certain number of things. But, nonetheless, you have been very very severe about his publications and his assertions concerning COVID-19.
OLIVIER BERRUYEY: [...] I disapprove of his having ceased to do science and medicine in order to do politics. He has politicised a subject that should have remained scientific. In order to prove that he was right, he abandoned the fundamental principles of medicine at a time when we needed them the most. He transformed the IHU Marseille institute into a lobbying centre for chloroquine. [Berruyey disagrees that Raoult's had a method of 'feeling one's way', describing it as] simply Raoult dedicated to proving that he was right, bit by bit. Systematically deconstructing any study that contradicted his assertions. Staying silent about a number of studies that showed certain dangers of the treatment, but carrying on about some extremely pedestrian studies, such as Professor Peron's, which was then withdrawn a few days later, and no-one talked about it anymore; and hiding the truth from people so as to make believe that chloroquin works. So, I demonstrated this in referring to scientific publications. I can do it here - it would take a bit of time - but people can look [for themselves]. I can cite a couple of little examples, which started off this chloroquin story. At the beginning of February, Raoul said, 'We have to listen to the Chinese. They are really the kings of virology. The Chinese use Chloroquin'. Terrific. So we must use chloroquin. After a month he said, 'We have to use hydroxychloroquine'. Hydroxychloroquine is close, but it isn't the same thing. The Chinese do not use hydroxychloroquine. Then he says, 'We're going to add an antibiotic, because that works better'. The Chinese guidelines say, 'If you use hydroxychloroquine, above all, don't use antibiotics because it is dangerous. And so, after a while, we find that Raoult says we should listen to the Chinese, but does the opposite. And, I will cite a second example which, to me, epitomises the problem: There was a study that showed that chloroquin seemed a little dangerous. Raoult said, no, it wasn't, and produced a small paper in response, drawing the reader's attention to a third study, which said chloroquine was not dangerous. Very good. However, after a comma following that statement, it said that, if you added an antibiotic - Raoult's protocol - it was very dangerous. It raised mortality. It's really pretty odd to have under your nose a study that says your protocol is dangerous, in order to convince people that your protocol is not dangerous. That's Raoult's method, in fact. It is perfectly understandable, because it's no longer science. There isn't any debate because 90% of scientists can see very well that it doesn't work, that there is a big methodological problem. But, obviously, there is a media problem as well, which tries to give the impression that if they look into it, that will be divisive. Scientists are not very divided. Someone with a doctorate in virologie, in biochemistry, who knows science, can see very well that there is a big problem. That's true overseas too. All the fake-science hunters have demolished this work.
RAPHAEL LIOGIER: I would really like to... The first thing is that to really look at it. In a way, my interlocuteur has validated what I said at the beginning. I said that Raoult works by feeling his way. Initially he said we have to follow the Chinese, then he changed his dosages, he changed the very nature of the product, going from chloroquine to hydrochlorothiazide. [sic] So, exactly - Raoul works pragmatically. And science has always been pragmatic; medical science especially. Medicine isn't physics theory. I have myself studied a little of the epistemology of medicine, and it isn't physics theory, it is, in fact, an almost artisan practice, where one goes from caring for patients to research, and from research to caring for patients. And Raoul functions within that paradigm. It is for that reason that he favours what he calls "observational studies" on the one hand, and going back and forth between them and caring for patients, on the other. It is in this way that he has progressively developed his treatment, which proves, in fact, that he is not maintaining a monological posture, only talking to himself and not with his team. No, he has progressively developed in his work whilst caring for patients - and I would remind you that the largest number of people tested in France proportionate to inhabitants is Marseille. He therefore had an enormous living lab for his practical studies, and he developed, little by little, coming to a point where he had the most efficient treatment possible. But I want to say a second thing, a second thing which is that what Didier Raoult was proposing cannot be limited to hydrochloroquine [sic], and I think that here, we are trying - it's a bit like the tree that hides the forest - we are trying to hide a certain number of errors. I think these are political errors. It's not a question of conspiracy theory, but of political errors by politicians. That's what took Didier Raoult well beyond the question of hydrochloroquine. [sic] Systematically testing everyone - and that's what was done in Marseille. You can reproach him what you will, but I assure you, it was what he could do in Marseille, as much as he could do with the means that he possessed - systematically everyone, and then to put to one side, that is, to put into quarantine, individuals who tested positive - and only them, only them. Then, after that, look after them, no matter the degree of their illness, and this with every precaution - meaning even when they were asymptomatic, and with every precaution - the precautions that are possible whilst using the drug hydrochloroquine mixed with azithromycine - but, as you said, my interlocuteur, doing scans, doing everything necessary, including systematically doing electrocardiograms. I went there, so I had an electrocardiogram. Everyone had an electrocardiogram. I was asymptomatic. So, taking every precaution. So, it was a methodology with everything together, of crisis management, second point. And the third point with which I would be in agreement, I think, and not completely with my interlocuteur, the third point, is that where there has been politicisation - but I am not sure that it came from Raoult. I think that there was politicisation from outside. Because, the only thing that Raoult did, if you listened, apart from his cheeky humour, his mind, his character [which was] a little direct. He might allow himself to say that it was a little bit of flu, etc. I'm not talking about that. Because, from a scientific point of view, he was a very serious person. I want to say that he was politicised precisely because what he was proposing was not just hydrochloroquine, it was a comprehensive strategy, opposed, in fact, to systematic quarantine. We don't know today if general quarantine was good. We don't even know if it saved lives or if, to the contrary, it caused lives to be sacrificed, when we look at societies like the Korean society, which did not practice systematic confinement, but which practised, as was proposed as a general method by Didier Raoult, systematic testing and quarantining of those who tested, and the act of caring for them, but which effectively reduced the circulation of the virus. Therefore, I believe, something quite rational and very pragmatic. But without that conceptual approach of seeking the perfect drug, because, whilst looking for the perfect drug, one finishes up sacrificing lives, on the pretext of claiming a kind of pure vision of what would have happened by the [indecipherable]. Medicine has only very rarely worked that way in the field of viruses and bacteriology. It didn't function that way with AIDS, which was frightening, and much more frightening in terms of numbers of deaths, of lethality, than the coronavirus. Why have we become obsessed with this today? Why has it entered into debate? I don't believe it's Didier Raoult who should be questioned. The question should be, why has Didier Raoult been the pretext of this, of these politicisations?
OLIVIER BERRUYEY: There is a lot to say. Amusing... We know that the people of Marseille were not put into quarantine at all, contrary to your [Raphael's] statement. Obviously, to stop an epidemic in the way that Korea did, is a very good example. You have to test to the maximum, from the beginning. We [the French] did not test to the maximum from the start, no more at Marseille than anywhere else because, at the time that we should have started testing, Raoult was saying everywhere that there would be fewer deaths [than from] scooters, and that all that was nothing particularly serious, that it was funny, really, and there was nothing to do, that [only three Chinese had died? - (indistinct)]. And so it was: when we needed to do something, we didn't do it. In effect, it's more problematic, when you finish up with millions of people infected, to do it. You can't dream of treating them. But, with respect to what Raphael Liogier said, would it be possible for us to agree on the fact that, today, we lack sufficient proof to say that there is clinical effectiveness and sufficient safety of use of hydroxychloroquine, not hydrochloroquine as you term it, with regard to managing COVID? Can we say today, at least, we don't know if it works?
FREDERIC TADDEI (INTERVIEWER): Raphael, Olivier has put a question to you.
RAPHAEL LIOGIER: So, I have three things to say about that. The first is that there was no quarantine in Marseille, but there were systematic tests, for the good reason that Didier Raoult does not have the police force at his service and does not have the powers of a state, in order to declare a quarantine and impose a quarantine on people. He is only able to look after them according to his ability, which is only a medical ability. So, that's a first thing. Evidently a quarantine required a political decision. That's precisely what I am criticising - on people who had tested positive, of course. On the dangers of the product. There is a difference between danger and effectiveness. I think that the proof of effectiveness, of absolute effectiveness of the product are not yet there. It's true that the only way to have formal proof of the effectiveness of the product would be to have randomised double-blind studies, etc etc. On the other hand, the proof we have today, with the backing away from this drug, which had been in free circulation for years, is that it is not dangerous if one takes a certain number of precautions - precautions which were taken. That's the first point. The second point is that, once again, the practical studies and the studies that were undertaken at the IHU institute on thousands of patients, show that there is a reduction in the viral load. I know that after it was said, "Yes, but there is other stuff." There is perhaps other stuff, but, whilst waiting for it, we have a death-rate that does not exist. And, not certainty, but an approximation of a treatment that reduces the viral load and which allows, at least at the start of the illness, avoiding passing on to the next stage. It seems to me that the statistics - although I know that you won't agree - since today this is the subject of controversy - but the statistics today in terms of mortality of infected people, seem less than in Marseille, at least in the people who have been treated at Didier Raoult's service - the 3 or 4 thousand people who went there, [compared] with the rest of France. [...] Therefore, for the moment, these statistics are effectively subject to caution, but I think that Didier Raoult was right to take that risk, for the good reason that he knew that by taking precautions, at least he was not causing the people he was caring for medically to run a risk. And thus, that the only possible risk, the only measurable one, might be to his advantage, according to what he knew. I believe that the matter is proven enough from that perspective.
OLIVIER BERRUYEY: What's proven is that Pharmacovigilance pointed to seven deaths and two hundred very grave side effects with chloroquine. In any case, it is not because you say so ... there is strictly not the slightest proof that the medication saves lives, nor that it reduces the viral load. The phrase that I cited before, saying that there is no demonstrated clinical effectiveness, was a phrase from Sanofi [Multinational Pharmaceutical Company and manufacturer of hydroxychlorquine] which was broadcast about 15 days ago, to every Belgian doctor. I repeat: To this day there sufficient clinical proof does not exist from which to be able to draw any conclusion about the effectiveness or safety of use of hydroxychloroquine in the management of COVID - that the manufacturer of hydroxychloroquine is telling you that it doesn't know if it works and if it causes damage. I find it amazing that we have succeeded in creating in France a world center for chloroquine lobbying, which manages to be far more extreme than its own manufacturer's. Furthermore, using techniques that even the worst laboratories would not use to promote their drugs. That's the problem. And, with reference to what you say, [...] The people of Marseilles are not macaque monkeys, nor things, on which, hey, let's look at this powder and see if it works, sniff this, gee, it's killing them. Lets test it a while to see and if there aren't too many deaths, maybe we can test it on animals. I mean, there were tests done on monkeys three weeks ago. Chloroquine with antibiotics, without antibiotics, at the beginning, before, after, the disease. It is ineffective for monkeys to date. It's all that. There's no 'feeling one's way'. Raoult's only subtlety is that chloroquine has to be given at 8am, or at midday. Should you give 600mg or 550mg? He's not asking, does [unclear] work or does plasma work or does interferon work? It's not respecting fundamental principles. It's taking a health risk, because it's not at all a [unclear] medicine. Hydroxychloroquine attacks the heart, somewhat, and so does COVID. When you add azithromycine, that also attacks the heart. A lot. That's why there are people who die of that treatment. As noted by Pharmacovigilance. These aren't things made to cause trouble or administrative regulations designed to prevent people being cared for. You said it very well yourself, Mr Liogier, the best thing is to have randomised double blind trials. To do a clinical trial you need a month. It's not something that takes eight and a half years. And, in fact, actually, the English did it; they didn't see any effectiveness, they just stopped testing hydroxycholoroquine, to go and concentrate on something else, other drugs. Because, when you say there aren't negative effects - if the greatest precautions are taken and one does echocardiograms every day, there probably aren't too many serious effects, I agree, but, in the whole story, over and above having attacked fundamental medical principles - and, I repeat, there is more need - listen, we lose time this way! Because, in the end, we have a raft of evidence - and I hope we will find the solution soon - I don't care - I hope it will work - chloroquine. I don't care, I am neither for nor against, but today there is a whole raft which demonstrates that it probably doesn't work because pharmacokinetics tells us that the dosage does not reach a sufficient level in the body to work. It has been tested on monkeys; it doesn't work. It has even been tested on the English; it doesn't work. And the tests on the people of Marseille, in terms of methodology, are ridiculous; there was never a control group, so one could not know if it works or does not work. We are losing time. If there is a second wave in autumn, we will attack it just as we did the first. There is no treatment. We have not tested interferon, we haven't tested lopinavir. Look, there are 50 molecules tested by [? unclear]; we have only talked about one. We have put all our eggs in the same basket. We must have had half the clinical tests in the world on that particular molecule. It's pretty staggering! There's no security for patients and it's not gone to the heart of the matter. I don't want -
FREDERIC TADDEI: Raphael Liogier has the floor. We have four minutes before the break.
RAPHAEL LIOGIER: Olivier, you know that today, most trials are not focused on chloroquine. They are focused on the others - It [chloroquine] is taking nothing from them. It's taking nothing from [trials] done elsewhere. I don't see why controlled use of Chloroquine in certain contexts would cost time. Why? I don't see the logic in what you are saying to me.
OLIVIER BERRUYEY: [Much crosstalking.] I will answer you, Mr Liogier. [...] All the media has said, for weeks, chloroquine is wonderful! Well, allow discovery to people. Come on, let us test Remdesevir on you. People said, 'No, I don't want any! I want chloroquine, and I don't want a placebo'. You have prevented recruitments [to other drug trials]. Stacks of media articles have described the problem very well.
RAPHAEL LIOGIER: I think it's a lot more complicated than that, what happened with the Discovery trials.[1] You are simplifying what happened with the Discovery trials. Furthermore, there was a series of trials undertaken using doses that were more than double those that were used at the Marseilles IHU. Responding to what you said about Sanofi - because you said a lot of things I need to respond to. On Sanofi - the fact that it wasn't conclusive, yes, I agree with Sanofi, as I said at the start. However, with regard to what you said about safety, you said there were seven deaths, until proof to the contrary, there is no certainty at all that death was due to any direct effect of chloroquine! And, moreover, the only effects that were able to be observed were relatively weak, and they can be controlled, they can be controlled, actually, by dosage, and they can be controlled, in fact, by - in certain extreme cases - by not using chloroquine - obviously. It's a medication which has effects, strong effects, and since those effects are strong, a certain number of precautions need to be taken - precautions that were taken. So, I say to you, you say, what was done in Marseille, it's vague, it's not serious, etc. All the same, thousands of people have passed through the IHU; hundreds have been cared for at the IHU, of which we have access to, whatever you say, we have access, I mean, through observation, to the progress of those patients- one can compare them statistically with what happened in other hospitals. We don't have - it's not yet conclusive, but it seems to me that it goes in the direction of the protocol that was used in Marseille. So, afterwards, one can say what one wants, regarding what Sanofi has said. You know very well that it doesn't constitute a proof. A laboratory can say whatever it likes; they are not scientific, even if they pay scientists. Besides, other interests could be involved, since Sanofi makes other medications, and it wouldn't be so profitable for Sanofi to sell hydrochloroquine, [sic] which is a drug that costs 30, 40, 50, 60 times less than all the others that are [unclear] proposed. So, I don't want to enter into conspiracy theories, but I don't think that your argument on 'the laboratory that says that... etc.' is a good argument.
[PROGRAM BREAK]
FREDERIC TADDEI: [summarises and asks Olivier Berruyey a question]: Olivier you said, in effect, that Didier Raoult failed to conduct a 'serious' trial in this area, randomised, double-blind etc. etc. He could have done it, you say. It takes a month. But, at the same time, we can see that no-one else did it either. In France no-one conducted that trial. Each time that we were told, 'Yes, someone is conducting a trial', either we never heard the results, or we discovered that it didn't have exactly the same protocol as Didier Raoult's. All that helped to strengthen the idea that there was a conspiracy against Raoult, against his treatment. Then some saw the reason that Rhaphael Liogier evoked, that it was a low cost treatment, and therefore undesirable, in the face of a preference for a very very costly hypothetical treatment that would present one day. But, for you, why hasn't anyone done serious clinical trials in France on this treatment?
OLIVIER BERRUYEY: Very quickly, very quickly, in effect, Didier Raoult did not conduct serious clinical trials, and I believe that he did not even conduct a legal trial, because there were problems with the legality of what he did, related to the primitive nature of those clinical trials, which are criminally punishable and [unclear] is dealing with this at the moment. We can see that the authorities have been completely lax on this issue. Why he didn't do it is very simple, because, when you do a trial, you have proof as to whether something works or does not work. In fact, what Raoult did, was to reject the method which would have subjected his assertions to a test of proof ... he knows very well ... but it's been a century that chloroquine, or quinine, from which it derives. People [?advocated] it as a treatment for flu; it wasn't. Every new era refers again to this resource. So, Didier Raoult, I understand very well, because he isn't doing science, he's doing politics. So, he wasn't going to do something that potentially would show him to be wrong. Why wasn't it done elsewhere? Yes. It is being done. The Discovery Trial in Europe, but its going very badly, because it is having difficulty recruiting, for the reasons I mentioned before. Look at the media coverage. There are many articles that explain that people wanted chloroquine and nothing else. The intention was to work out once and for all what was happening in France, but others said, let's involve other European countries. Let's do a European thing, with the Germans, with the Italians, with Spain. It will be wonderful! -- Finally only Luxembourg joined the study. I think they only had 10 patients, what's more. So, the thing was completely ridiculous. Macron promised us the results for the 13th of May, so, ride the tiger, it won't be long. On the other hand, however, maybe due to Brexit, the English did manage to test it. Their test showed that a double dose of chloroquine was ineffective. It is therefore very strange that Liogier again took up that argument. 'Look, people tested it at double the dose. That's the reason it didn't work'. It's beyond ridiculous.
FREDERIC TADDEI: There was a review planned by the Angers CHU [Centre Hospitalier Universitaire], wasn't there?[2] I said to myself, we can tell people about it during this program. We will know the answer then. It won't be necessary after to have friction between believers and unbelievers; between for and against Raoulters. We'll just [unclear - refer to?] the Anger results. What happened to it?
OLIVIER BERRUYEY: It was a lamentable government mistake. We agree. There was no pilot. That business was in the image of -
[Both talking over each other so Unclear.]
FREDERIC TADDEI: Why, in that case, would [French President] Macron go and visit Raoult? Was it because he doesn't want to cut himself off from all the French who believe in Raoult? Is this demagogy?
OLIVIER BERRUYEY: I don't know. Because Macron is anti-system, as he says. And there will be anti-system people there. And, with all these anti-system people, they will argue between themselves. [Laughs.] It's lamentable. Truly lamentable.
RAPHAEL LIOGIER: Well, to begin with, I don't know why it would be a ridiculous argument to say that one doubled the dose. You must know what the medical word, 'pharmacon' means? In Greek, it means what? It means something that both poisons and treats. So, that means that dosage, in medicine, until otherwise proven, is a fundamental variable. Therefore, an absolutely fundamental variable. It's not a detail. It's not at all funny. To have given a double dose - that could be totally counter-productive. Therefore -
OLIVIER BERRUYER: [Shouts and makes exaggerated feeling with hands out motions:] He's feeling his way! Feeling his way! He's feeling his way. He's looking.
RAPHAEL LIOGIER: Don't get excited. Calm down.
FREDERIC TADDEI: [Laughing silently at the spectacle.]
RAPHAEL LIOGIER: You know perfectly well, that if you take aspirin, even aspirin, you can kill someone by increasing the dosage. Even more so with [? azithromycine]. You know very well that dosage is actually important. Especially a double dose. You yourself have argued as if it's a medication that should be handled delicately. To double the dose, I believe, is a major [unclear]. Secondly, I find the argument interesting, what you are trying to do here: That Didier Raoult is politicking. I don't see in what way Didier Raoult is doing politics. I think this is a way of attributing a kind of conspiracy theory. If Didier Raoult has not done double-blind randomized etc studies, this would not be because we are in a crisis, and an emergency, would it? You look after people before you do controlled experiments, don't you? It wouldn't be for that reason, as I believe it is? There's crisis, a time of crisis, and there's a time for research, at another rhythm. And I am in agreement that the two may work without excluding one from the other. But, instead of thinking this way, people project onto Raoult some kind of malign intention, since you say, 'He wouldn't have, because that would have proven that ...' So, why has he become so attached to hydroxychloroquine? Why, when it doesn't work? Because he is absolutely bent on proving that it does, so he had a malign intention? He makes the people he looks after take a risk - and his patients' opinion, I mean patients he has taken care of, whose opinion is important, until proven otherwise - after all, no legal suite has been launched against him to date, and I don't think that every doctor in France and Navarre could say as much. There is no legal matter against Didier Raoult in Marseille today. It's not because the people of Marseille are more stupid than others; it's because they feel looked after; those who were touched have felt it in the first degree. As for me, I cannot understand what can be Didier's interest - what is the conspiracy theory that supposes that Raoult's obstinacy is politically motivated? That is, hydroxychloroquine as a political weapon for Didier Raoult. Why? In order to become mayor of Marseilles? To be elected President of the Republic? To get the Nobel Prize? But he won't get the Nobel Prize, of course. You say that you are sure that ultra-serious trials will prove that it doesn't work. Then he is sure, at that moment, to hit the wall and not win the Nobel Prize. So, what he is, you are saying is - conspiracy theory - intentionality, and, furthermore, he is stupid, because, as it will be revealed, he will fall on his face. Which one is it? Either he's an extremely intelligent bloke, in a conspiracy theory, or he's completely stupid. You want both at once. It's contradictory. You can't have both at once. So, I don't understand your relentless desire to politicise Raoult's discourse, when he is just behaving like a doctor in a time of crisis, in an emergency situation. And, until there is proof to the contrary, the patients he takes care of, who are massive in number, well, I believe they are quite satisfied. That's not bad. He hasn't killed anyone.
OLIVIER BERRUYER: At the IHU there are 75 places. Is that right? There are 75 beds?
RAPHAEL LIOGIER: [Nods.]
OLIVIER BERRUYER: You aren't contradicting me? There were 36 deaths.
RAPHAEL LIOGIER: Yes. Exactly, 75 beds. - No, no! [in response to the 36 deaths statement]
OLIVIER BERRUYER: Raoult finished up saying it at the [?United Nations/United States]. That's all I'm saying. There were 36 deaths and 85 beds. Already it seems to me that they weren't very happy. There, you see. Second point:
RAPHAEL LIOGIER: No! No! 75 beds, I agree, but -
FREDERIC TADDEI: Let Raphael Liogier speak. He is a member of the Ethics Committee, after all ...
RAPHAEL LIOGIER: 75 beds reserved for urgent cases who must enter those beds according to very specific conditions, you know, because they are very expensive - there are very particular hygiene conditions, in order to manage a patient in a bed at IHU. Therefore, the patients stay a very short time, then move on - the next kind of care occurs in the main part of the AP-HM [Hôpitaux Universitaires de Marseille], in the [?], sometimes even in other hospitals, or sometimes people go back home. The 75 beds are a place of transit, in fact, thousands of people have been through them, since the beginning of the crisis. 75 beds, it's just a place of transit and for - how can I say it - extreme cases, exactly.
OLIVIER BERRUYER: Okay. It's not a place of transit. Most people who are treated - there are more than 3000 - have not been hospitalised. Those people were ambulatory, they were not - at any rate, there was nothing wrong with them when they were examined for symptoms. And even asymptomatic. There were 36 deaths. So, then, give us the number of hospitalisations that occurred before there were 36 deaths. That interests us. Do the ratio. You like ratios; you are a statistician. So, little statistical manipulations; [? one can't do too many of them.]
RAPHAEL LIOGIER: I am not a statistician! I don't know the exact numbers. But I know that up until then, and until proof contrary, there have been no complaints, individuals who were displeased with the treatment, and the deaths to this point which have been accounted for - I'm not a doctor, but we will see - [?unclear] were not deaths, until proof to the contrary, due to treatment there, but due to what is called co-morbidity - a whole series of things. What counts - since you are a statistician - what counts - and, in the end, it's that which we will look at - is the number of persons treated, not just hospitalised, in the IHU - because, to be precise, they pass through the emergency part, intensive, because they are in crisis, and, after that, their place becomes available for someone else. What is important to know is, on the total of people treated, who may or may not have been hospitalised - if the illness did not require hospitalisation - to know what the statistical ratios are in terms of mortality, aggravations, or people who left. It's that alone that will give us the data, and we will have it. We will have it, necessarily. I believe that the [ratios] are to the advantage of the IHU, for the moment.
FREDERIC TADDEI: It was believed that we had that data when the Lancet, the prestigious scientific review, published a study that tended to agree with your critical work, Olivier Berruyer, since it was said that, looking retrospectively, several tens of thousands of patients, who had been treated just about everywhere in the world, once could conclude - and that is what this study concluded - published in the Lancet - conclude, not only that this treatment was ineffective, but moreover, it was dangerous; it added to the mortality. And, it was, besides, following that publication, that the WHO [World Health Organisation] said that it would be better not to use hydroxychloroquine anymore, and, in France, its use was forbidden, therefore, as treatment. And then, boom boom, the next day, or the day after that, the Lancet itself backpedaled and warned against what it had published the day before. And we noticed, and we were told, that data had been falsified, etc etc. How do you explain that, Olivier Berruyer, because you must have read it, this study, you must have thought it backed you up and then, the day after, that it didn't.
OLIVIER BERRUYER: No, no. Not at all. At no moment did I take a position on chloroquine. I don't know if it works. There is only one way to find out if a medication works - you need to do a double blind randomised trial. And then you will know if it works or not. I have never said on my site whether it works or does not work. There are studies that say it works, when it's not true. So, that's the Raoult problem. I don't say that hydroxychloroquine doesn't work. I say that, when Raoult says it works - and he said it from February, in February, he said, it's good, we've found the remedy and COVID will be the easiest respiratory infection to treat. I repeat his words, and 400,000 people are dead. Perhaps we will not have a remedy and that's something that people are not about to accept. There may never be a medical treatment, because generally viral illnesses don't have treatments. There's no treatment against measles, against rubella, against flu. It doesn't exist, so, there's no obvious treatment. Simply, when I saw the Lancet - to go back to the subject, the conclusions went in the same direction of five or six preceding studies; it wasn't a revelation. In effect, its statistical power was interesting, for having a beginning of an answer. [The study] in the Lancetconcluded by saying, 'Now, it's not sure, we need to do a randomised double-blind trial'. It was not categorical on this point. Anyway, globally, that the Lancetgot caught up in all these politics was quite astonishing. It's proof that there is fraud in science, of course. That's the reason we have [? unclear] ethical; that's why we have fraud-hunters. I'm not against Raoult. I'm against bad science. It's just as disgusting what Mehra [presumably Dr Mandeep R.Mehra, the leader of said study that was withdrawn] did, as what the Lancet did. Them and Raoult's bad science. So, we really have to organise ourselves, we surely need to do major reforms, on pharmaceutical laboratories so that there will be less lobbying at that level, on public research, and on the publication of data, umm... I'm not going to elaborate further here, but there are lots of things to do.
FREDERIC TADDEI: After the final rebound on the study in the Lancet, against which the Lancet itself has warned us, what conclusion have you drawn, a part from the fact that we are always in the shadow of belief, aren't we? Whether we are for or against, Didier Raoult. It's passion and it's blind.
RAPHAEL LIOGIER: There, yes. We are testing, but we are blind, in fact. We have blind conclusions. [Laughs.] Even if, in effect, the Lancet article, as the New England Journal of Medicine, which are two big medical journals that published the same information, are not entirely conclusive. For me, what I find fascinating - and I agree with my interlocuteur - is the politicization that has taken place, a politicization - and I imagine that you would agree with me saying, how is it that reaction to the only article in a serious publication (putting aside the standard of the article itself) has been an almost immediate reaction by the WHO and the French government? This is irresponsible on the part of Raoult's critics, who call him inopportune, but I think that what they did was inopportune, in the real sense of the word, meaning, 'ill-timed'. I mean that it was extremely rapid, as if an immediate reaction was needed. That's the first point, because there, the politicization is very real. And, the second point: These scandals make it seem - because it's over and above the question of chloroquine, over and above the political question of Raoult, for or against, and all those things - make it seem as if, today, research in medicine particularly - there are problems today in medical research - how should I say it? In the financial links of laboratories - because we know that it is partly linked to that - the [unclear]. I mean financed in order to go faster, in order to impress - since we are talking about statistics - impressing by having extremely wide statistical samples, using artificial intelligence to process them, via a start-up - we don't really know that start-up is serious, if it exists, if it even exists, for as long as it has done what it has done, how it did it. We discovered, little by little, that even Australian hospitals had not given the figures that they were presented [in the study] as having been received. There were even errors where an Asian hospital was counted among Australian ones. To sum up, it was - Imagine, imagine the other way round, just for a second, what would have happened - we saw what happened there - Imagine what would have happened if such a mistake - I mean such a scandal - had occurred in the setting of the emergency management choices that Didier Raoult might have made in his IHU. He would have been literally crucified! Because truly, the article - I mean it's almost never happened - [...] I had never seen, at any case, in the Lancet [...] even the head director of the Lancet had already criticised his publication editorially in certain articles - but, to such an extent? It had never happened. A questioning of the actual credibility of the most prestigious scientific medical journal in the world, the one that is supposed to represent the greatest guaranties, I tell you, followed by the New England Journal of Medicine. It is truly extraordinary! Truly extraordinary!
FREDERIC TADDEI: We need to be clear that there have been previous retractions by great journals like the Lancet. And, as Olivier Berruyer said before, more and more falsification. I remember two books on that problem, which increases every year because researchers are obliged to publish in order to justify the money they ask for, therefore publishing takes place at greater and greater speeds, and sometimes the data is a bit manipulated to make it fit one's case. All the same, a retraction -
[two people talking at once]
RAPHAEL LIOGIER: In science it impacts even more, because it isn't only publishing in order to publish, like us in political science, it's because it is necessary to publish immediately, because [the research] was financed by a laboratory that wants immediate results, so as to be able to proceed more quickly towards commercialisation of its drug. I think that's it, really. It's undeniable; I'm not slinging stones at anyone. There are direct links between finance, pharmaceutical laboratories, and what is called 'basic research'. It's undeniable.
FREDERIC TADDEI: Olivier Berruyer, given that this has been a recurring accusation during the entire Raoult business, this accusation against big pharma, the pharmaceutical industry, and its links with a number of doctors who would then be anti-Raoult ...
OLIVIER BERRUYER: I feel that it's a rather sad business. Obviously there's a basic problem, and I'm not pro-big pharma. I think that we should nationalise Sanofi because it isn't right that we lack a public laboratory for the production of medications. I think that we should forbid remuneration of doctors by laboratories. I think we absolutely need a public organisation for publications. Okay, that's all true, but there are also problems with the public system. For instance at the IHU of Marseille, where Raoult started signing 150-200 studies a year, when a quality researcher only publishes about 100 in his lifetime, normally. This makes Americans laugh, knowing that each time colleagues who have organised themselves at Marseille, publish in a review, it means that 600 euros go to the AP-HM, to the detriment of other hospitals in France, for which there is also a big problem with public finance and that method of finance, which has been very strongly criticised by the Court of Accounts [French supreme auditing institution]. I dare to hope that the government will act on this point. Yes, there is a problem, and it needs to be treated. Now I find it regrettable that side of things that consists of saying, 'Yes, but any doctor in a situation of conflict of interest is an untrustworthy creep, a low-life, whom you should not listen to.' I repeat, I don't like this system, but you should not conclude that just because there is a financial conflict, that shows that you should look more closely at the case against that person, just because they have a conflict of interest. It doesn't mean that what they say is false. And conflicts of interest are not only financial. There is also the Marseille IHU conflict of interest. It's obvious. Mr Raphael Liogier is trying to tell me that there would be no problem if Raoult were to say, 'Hey, I made a mistake. I've just treated 3000 Marseille people for nothing. Chloroquine doesn't work at all.' It's true that it is going to be very interesting in a few months, alas, if scientific truth concludes this. [...] To conclude, as Mr Liogier does, that when Sanofi says that chloroquine doesn't work, it's possibly -
RAPHAEL LIOGIER: [Interjects]
OLIVIER BERRUYER: [Laughing and waving finger] Yes, yes, I think you did say that. You said that, even when the laboratory says its own drug doesn't work, to try to get out of it - when normal logic would [conclude that the drug] doesn't work - [by saying], 'But no, perhaps they are hiding another drug, which they can sell for a higher price.' Meaning that those involved prefer that we die without treatment. That's it. This is dirty reasoning. And that a philosopher could think that, could introduce that idea to the population - and we know that the population will easily react to such a shocking kind of thing
RAPHAEL LIOGIER: [Softly] No, no, no, no.
OLIVIER BERRUYER: I find it very shocking. We can go over that bit in the recording. I'm not fussed. That's exactly what you said.
RAPHAEL LIOGIER: Fine, we'll go over that bit in the recording. I'm not fussed either.
OLIVIER BERRUYER: But it's the little refrain that
[Liogier and Burruyer talk over each other.]
OLIVIER BERRUYER: Yes. Okay, I'll take that on. It's of little importance.
RAPHAEL LIOGIER: Don't say it's of little importance.
OLIVIER BERRUYER: But what importance does it have?
RAPHAEL LIOGIER: Don't say it's unimportant. It is important. I think what you said is important.
OLIVIER BERRUYER: You have to find the sweet spot. Of course, you have to doubt, of course there are conflicts of interest, of course you have to be careful, but afterwards you find yourself in a world where you imagine that everyone is surrounded by untrustworthy creeps who aren't telling the truth and who... Hey, when I think of the number of doctors who have bust their guts throughout France [and] there's an attempt to make us believe that Raoult is fighting a war for medicine ... but all doctors have tried it - Even the Salpetriere [major teaching hospital in Paris] used it from the outset, since the Chinese used it. I've talked to doctors at the Salpetriere, and it's not the only thing, Raoult is not the only one doing it - all the doctors are busting their guts; you have 15-20% of the medical corps who have caught COVID. That's too many. To try to make them all out to be low-lifes and sell-outs, all of them - it's too many - to cultivate that sort of - I don't like the word, 'populism', that sort of [?bitter opinion] to conduct polls-
RAPHAEL LIOGIER: [Interjects] I didn't say that -
OLIVIER BERRUYER: But many have said it. You didn't say it, but many have in that fringe-thinking. I find that - I don't see how we can construct a decent world if one thinks that way and, if, furthermore, one has different realities. One can no longer agree on basic facts, when Science normally allows us to do that.
FREDERIC TADDEI: Raphael.
RAPHAEL LIOGIER: Okay. Firstly, on Sanofi, I absolutely did not say that they were low-lifes, that they wanted to sacrifice peoples' lives to profit etc. I'm only saying that, when you give as an argument [that] chloroquine doesn't work - the proof you say is that Sanofi says so - is not at all an argument, a laboratory that says something works or does not work, even if the same laboratory manufactures that particular medicine. That's what I wanted to say. Because I am not at all into conspiracy theory and I'm not at all inclined to the idea that the world is full of low-lifes. I believe there are interests, but multiple and variable interests: we have an interest is being cared for, an interest in being happy, an interest sometimes in earning money, and all that is very complex and multiple. I don't believe in an intentional malignity. So, it wasn't a perverse argument. It was just to say that there is no proof for [the argument] you have advanced -
OLIVIER BERRUYER: Yes, yes.
RAPHAEL LIOGIER: - that it's because of what Sanofi said.
OLIVIER BERRUYER: Of course. There is only blind clinical testing, that's the only proof.
RAPHAEL LIOGIER: That is true. I am even in agreement with you on that. But I believe, on the other hand, that practical international studies in crisis situations, in pandemic situations, over a long time - over a short time! - excuse me! - are not at all incompatible with tests in [unclear] and, contrary to what you say, do not slow down research. But, as far as the number of important articles by Didier Raoult is concerned, I'm letting you know that this also happens in America, but I am an invited researcher at Columbia University, which has a very, very, very big medical school - of medical research - and I assure you that the [?unclear] there, the really big researchers, well, they also put their names on many massively published articles. Then, money doesn't go to the AP-HM, it goes to the IHU Foundation - yes, it's not the AP-HM.
OLIVIER BERRUYER: It goes to the AP-HM, it goes to the AP-HM.
RAPHAEL LIOGIER: Nooo...
OLIVIER BERRUYER: No, no, not directly. Into the pockets of -
RAPHAEL LIOGIER: It doesn't go into Raoult's pockets...
[They continue to contradict eachother for a little while]
OLIVIER BERRUYER: At any rate you haven't published the accounts. You haven't published anything on your figures on your internet site, therefore ... It would be good, besides, if you would do that.
RAPHAEL LIOGIER: Wait! Wait, just a second! I am not a representative for the IHU! I don't know the IHU's [financial] curves, I am a university professor in political sciences, and I am a member of the Committee of ethical supervision, and my position stops there. And no more than that.
FREDERIC TADDEI: This show is about to end. I propose that you each conclude with a few words - if it's possible to conclude anything in this business, when there will certainly be comebacks. Olivier Berruyer, on this business of Didier Raoult:
OLIVIER BERRUYER: It's a rather special business because usually you can have doctors who try to fool other doctors and scientists. Here we have someone who has come out and who is more preoccupied with what other scientists think of his work, in order to get opinion to support his side. He has succeeded rather well in this. [unclear] Raoult's method; Raoult's refusal of the scientific method is nothing new. It has happened before. It is Moliere's vaccine. Hey, here comes COVID, blood-letting for everyone! Let's test, but, above all, don't separate the group into those that are bled and those that are not. In any case, we've been bleeding people for 200 years so, if it didn't work, we'd know it. It's exactly that, this method that rejects science. It's a method that rejects proof and it refuses respect for the patient, who is not a guinea-pig.
FREDERIC TADDEI: Raphael Liogier's response?
RAPHAEL LIOGIER: Well, it's funny, because I find that it's exactly, in a sense, symmetrically the opposite. It's symmetrically the opposite, meaning, to offer a patient a strategy that does not pretend to be unfalsifiable, is pragmatic. It's rational and pragmatic. Pragmatic because rational. And, if there were, in fact, problems, well then, it would stop. If there were [problems] then [the treatment] would stop. That would happen through observation of the patient by the doctor. When one is operating on a scale of thousands of patients, the problem is inverted. The problem of randomised trials is that theyseek a pure, an absolute, medication, which you have said yourself may never be found. Well, it's through waiting, as long as the perfect medication, the unfalsifiable medication, has not been found, in some way, then you are sacrificing the population. Sacrificing the population, in a way, by calling on a kind of positivist theology of ideas that it is absolutely necessary to find the corresponding medication, but without going as far as Moliere, because that's a false criticism, because, in that era, it was more or less magic. It is in fact - euh - medicine is not a science like the others. It is a science which supposes what is called the unique dialogue, which means a special relationship with the patient, which therefore evolves. This is, in effect what Didier Raoult practices, without this implying any opposition to basic science.
This interdiction was modified in July 2020, so that Plaquenil (brand-name for hydroxychloroquine) could again be prescribed. However, the French national health scheme would not reimburse prescriptions for its use outside traditional indications, like malaria, lupus and arthritis. It could still be used and prescribed for other purposes, including COVID-19 treatment, as long as this was stated on the script, but in such cases, the government would not reimburse the script. See
>Non, l'hydroxychloroquine n’a pas été "réautorisée en douce par le gouvernement Castex". See quotes below in English and French:
"However, it states that Plaquénil may be prescribed outside its marketing authorisation, as provided for in the Public Health Code, provided that "this is justified by scientific knowledge and that the patient is clearly informed". "In this case, it must be mentioned on the order and it will not be reimbursed", noted the DGS stressing that "in case of problem, the civil, criminal or ordinal liability of the doctor can be engaged." (Translation from: "Elle précise toutefois que le Plaquénil peut être prescrit hors de son autorisation de mise sur le marché, comme prévu par le code de la Santé publique, à condition que "cela soit justifié par les connaissances scientifiques et que le patient en soit clairement informé". "Dans ce cas, cela doit être mentionné sur l'ordonnance et elle ne sera pas remboursée", a relevé la DGS soulignant qu'"en cas de problème, la responsabilité civile, pénale ou ordinale du médecin peut être engagée."
With COVID-19, we should not just be looking at deaths. Deaths may actually be a poor indicator of the damage this virus may do. We should be looking at a continuum, as in: If the proportion of people who contract COVID-19, and who are over 80, die, what happens to those (of any age) who live? Given the ability of this disease (unlike flu) to cause clotting problems all over the body, affecting organs which affect other organs, we should be expecting that a proportion of survivors will have various rates of blood clots and organ damage. What proportion of these will clear, improve, or become chronic and dangerous? How long will how many survivors survive? Check out the following videos by doctors regarding clotting and organ-damage.
[Candobetter Ed: This article was developed from an extract from another, in order to highlight these concepts.]
"More long-term damage caused by COVID-19 than expected | COVID-19 Special" (August 26, 2020)
The above video has many comments of interest, from people who have suffered lingering damage from the virus.
"An NYC Cardiologist Explains the Long Term Effects of COVID-19."
The cardiologist in the above video points out that, even if you are young and fit when you catch COVID-19, you still may not be able to do what you used to do, after you recover. He also says that people should present early for treatment because then treatment can be started to reduce the damage to organs, thus perhaps reducing the severity of chronic conditions that may linger and prevent full recovery. He also says that four years after the 1918 Great Flu epidemic, many survivors still had debilitating symptoms.
"Long-term health effects of COVID-19" (Lung specialist talks about pulmonary fibrosis, which may lead to need for lung transplants.)
Most important to factor in, among all these continuum possibilities, is the incredibly infectious nature of COVID-19, far more than the flu. Cummins does not appear to think much about this.
Perhaps it would be more useful and educative to describe COVID-19 as a clotting disease, than as a respiratory one.
Ivor Cummins is a health writer and biochemical engineer, who calls himself The Fat Emperor. He has drafted a letter for people to send to politicians and the press, querying the seriousness of COVID-19. He calls it the "Corona Basic Realities Letter," and writes, advocating 'herd immunity', as one of his 'indisputable facts', that: "Sweden, who were vilified for their approach, has had a very similar death rate to other countries." But Sweden actually has had a much higher death rate than its neighbours, although it did practice social distancing and other hygiene measures, whilst leaving businesses open etc.
The virus killed more than 5800 people in the relevant period, giving Sweden one of the world’s highest per capita mortality rates.
To compare those figures with other Scandinavian countries, Denmark has recorded 621 deaths, Finland has recorded 334 deaths, and Norway 262." [Sweden has about twice the population of the other Nordic countries, but the number of deaths is still very high in comparison.]
"The study, carried out by the country’s Public Health Agency, found that just 6.1 per cent of the country’s population had developed coronavirus antibodies by late May. This figure falls far short of Dr Tegnell’s prediction.
Cummins compares South American countries, Peru vs Brazil - lockdown vs none - claiming death rates are similar and assuming this proves lockdown does not help. But he should take into account other factors, such as dirty water, crowding, poor hygiene, undocumented workers, poor health system, which would make lockdowns and or treatment ineffective. See https://www.kunc.org/2020-08-31/peru-grapples-with-the-pandemic-despite-an-early-and-tough-lockdown.
Cummins criticises (Ferguson's epidemiological model> (an early influential British coronavirus epidemiological simulation that contributed - among others - to lockdown decisions), for Sweden vs 'actual' data. Strangely, Cummins does not appear to take into account the effect on the death rate of measures taken against the virus in Sweden, albeit lesser measures than in neighbouring countries (which had much lower death rates). This virus is so infective that, without any infection control measures, much higher contagion would be expected. This seems to be a common error in criticisms of quarantines and lockdowns. See this article for a thorough explanation of what the Ferguson model purported to do.
Ivor Cummings does not talk about Italy, which is an example of an entire country crippled by COVID-19, with a high severe illness and death rate that overwhelmed the hospital and funeral system. Three well-known factors operated there: The first was a mass infection that took place in a crowded football match; the second was that the government treated COVID-19 as if it were no more serious than the flu; the third was that Italy had such a high proportion of elderly people. The situation was made worse by the government failing to give financial support to its citizens, whilst ordering them into lockdown.
Victoria, Australia, is still experiencing in September 2020 what most of the world would see as a comparatively minor outbreak of COVID-19 in the community – certainly in contrast to Italy. The state initially locked down the most affected suburbs, but expanded lockdown quickly to the rest of the metropolis, and some affected regions. Contiguous states locked their borders against Victoria. Known new infections only reached 684 at their current peak, against a background of total known infections of 19,688 total, yet contagion reduced hospital and nursing-home staff, by quarantine and illness, to the extent that other states had to send in relief. What would have happened if there had been no lockdown? The virus would have spread to all other states and the hospitals would quickly have been overwhelmed. If, bizarrely, staff had continued to work in them without being tested themselves, without isolating if asymptomatic, patients presenting to hospitals with other illnesses would have run high risk of acquiring COVID-19 in addition to their presenting illnesses. Knowing this was a risk, even with quarantine, people avoided hospitals. Victoria is not out of the woods yet, and a small number of infections have escaped beyond the state, but the health system has coped to this point.
Cummins seems to be championing the idea of herd immunity, without thinking it through. Herd immunity needs definition. Many definitions disagree. The requirement, in herd immunity, for a much higher number of cases to establish, than usually allowed through strict quarantine, would mean potentially far more suffering. The virus would not go away, but would remain in the community to affect upcoming aging or otherwise vulnerable cohorts; thus a lurking endemic nasty. The capacity for COVID-19 to reinfect, and the ability of the virus to change rapidly, calls into question the very possibility of widespread immunity.
Not just deaths
Cummins should not just be looking at deaths, and neither should we. Deaths may actually be a poor indicator of the damage this virus may do. We should be looking at a continuum, as in: If the proportion of people who contract COVID-19, and who are over 80, die, what happens to those (of any age) who live? Given the ability of this disease (unlike flu) to cause clotting problems all over the body, affecting organs which affect other organs, we should be expecting that a proportion of survivors will have various rates of blood clots and organ damage. What proportion of these will clear, improve, or become chronic and dangerous? How long will how many survivors survive? Check out the following videos by doctors regarding clotting and organ-damage.
"More long-term damage caused by COVID-19 than expected | COVID-19 Special" (August 26, 2020)
The above video has many comments of interest, from people who have suffered lingering damage from the virus.
"An NYC Cardiologist Explains the Long Term Effects of COVID-19."
The cardiologist in the above video points out that, even if you are young and fit when you catch COVID-19, you still may not be able to do what you used to do, after you recover. He also says that people should present early for treatment because then treatment can be started to reduce the damage to organs, thus perhaps reducing the severity of chronic conditions that may linger and prevent full recovery. He also says that four years after the 1918 Great Flu epidemic, many survivors still had debilitating symptoms.
"Long-term health effects of COVID-19" (Lung specialist talks about pulmonary fibrosis, which may lead to need for lung transplants.)
Most important to factor in, among all these continuum possibilities, is the incredibly infectious nature of COVID-19, far more than the flu. Cummins does not appear to think much about this.
Ivor Cummins' letter suggests that recent rises (second waves) of corona virus are the result of countries conducting more tests, or the effects of seasonality. There seems to be little evidence of seasonality, however.
He speaks confidently of vaccines to help the susceptible, but there is no certainty of any effective vaccines arriving.
Innes Willox, the Chief Executive of the Australian Industry Group or AIGroup, aims to bolster the economy by resurrecting the discredited mass-immigration agenda. His group has been described as: A leading organisation representing business in a broad range of sectors including manufacturing, defence, ICT and labour hire, by the Australian Advanced Manufacturing Council (accessed 1 September 2020), which lists him, among other positions, as “Board Member of Migration Council of Australia,” and notes that he “was Chief of Staff to the Australian Minister for Foreign Affairs, Alexander Downer, from 2004 to 2006.”
To appreciate the agenda, in the article, Migration, tax reform a key to revival, (Geoff Chambers, The Australian, 24 August 2020). Chambers wrote that the Australian Industry Group was calling for “a long-term, systematic shake-up of the tax system focused upon the removal of the worst taxes.”
But the overriding aspect of AIGroup’s push requires the Federal government to achieve,“An increase of the migration cap.”
Innes Willox, repeats his decades-long mantra:
“Restore the migration cap to 190,000 places a year and [furthermore] move to [implement] a growth rate target for annual permanent migration [levels, because] migration was critical to Australian prosperity.”
Willox and, indeed, that coterie of like-minded Big Australia cohorts, construe that merely importing copious numbers of immigrants will bolster ‘demand’. Therefore, the sacrosanct supply and demand factors which economic-rationalists embrace, will summarily kick-in - and boost economic growth. It all seems so straightforward and logical.
There’s nothing there about what might happen when these immigrant groups become so large that they could use their numbers to establish political entities to organise for their own benefit and possibly against Australia’s!
Of course, this disaster already seems obvious to many. Rancour inside the major parties shows it. In Victoria an Indian woman in the Liberal Party has established a ‘religious Right’ faction based on certain migrant groups. In South Australia a Chinese woman and upper-house MP is openly advocating for China and Chinese migrants. Are we surprised?
Without doubt, Innes Willox and Co would gloat about this scenario, as being culturally diverse and enriching. When, in fact, what it really is cultural separatism; if not downright divisive. And this is evident in that, outside workplace requirements, many in the array of ethnocultural groups in Australia, rarely interact with those outside of their cultural-bubbles. Except, perhaps, as Clive Hamilton, in Silent Invasion: China's Influence in Australia, argues, they seek to flatter and influence people holding political and business positions.
At any rate, Australia’s Prime Minister has reacted, introducing legislation requiring Federal oversight of any agreements with foreign powers/investments: “The government will introduce legislation next week empowering the foreign affairs minister to review and cancel agreements – such as Victoria’s decision to sign up to China’s belt and road initiative – if the commonwealth judges the arrangement adversely affects Australia’s foreign relations.” See, Victorian premier defends China deal as PM pushes to override state pacts with foreign nations. On the other side of the coin, many Australians continue to worry about Australia’s role as an international deputy to the United States war machine. (See, for instance, The Independent and Peaceful Australian Network, “Don’t buy into war.”). Most of us can probably agree that we would rather be independent and sovereign.
In past times, advocates of open-door immigration programs claimed this would enrich Australia. Alas, what has transpired is that immigrants had arrived in such droves, over the past decade, that they have rapidly displaced established Anglo-Celtic-European ethnicities from scores of suburbs in Sydney and Melbourne. The end result more closely resembles a collection of peoples, with diverse national or ethnic allegiances, rather than those of what once-was, termed ‘mainstream Australia’.
Further, over the past few months, we’ve seen the Big Australia advocates, like Willox and the AiGroup, calling for the government to fast-track international students in Australia from temporary migrants to permanent residents, as the stepping stone to fill job requirements. The effect of this would be to counter the drop in immigrant numbers which has followed from COVID-19 closing the borders to foreigners. What manner of gross-insanity exists here, with them demanding international students fill the void, when unemployment presently stands at 14% and underemployment is at a comparable percentage?
Willox reportedly purports that
”Immigration was critical to Australian prosperity and the pandemic has necessarily constrained inward immigration, but Australia would need to think long and hard before any decision [was made] to sustain lower levels over a longer term and the reduction in permanent migration visas had contributed to a reliance on temporary migration flows, dominated by students and backpackers. (”Coronavirus: migration, tax reform ‘key to recovery’”.)
Clearly, what Willox and AiGroup’s long-term migration strategy entails is summed up in the following two statements:
“[Australia’s future prosperity] would be enhanced by moving to an annual growth rate target for annual permanent migration that is linked to [the] national labour market growth, instead of a fixed quota number.”
“The changed outlook for immigration has huge implications for many industries, especially of immigration in housing and construction, which have been fueled by high levels both permanent and temporary levels.”[Emphasis added]
Well, taking into account that immigration intakes into Australia between January 2014 until June 2019 were, comparatively, 2.25 times higher than that of the US, prompts these queries:
If, as Willox and his cohorts claim mass-immigration makes Australia richer, then how come we are the most indebted society in the world? Surely, if the theory espoused by Willox and all of the Big Australia Brigadistâs is correct then prices/costs should, at the very least, be stagnant? Unlike as over these past 75 months during an era of huge immigration levels - since the LNP won office in September 2013 - house prices have increased by 60%, but wages only rose 15%?
Clearly, in spite of the relentless-claims made by the Big Australia Brigade, open-door immigration into Australia, hasn’t made us wealthier at all. These policies have actually encumbered the country with the exact opposite scenario. Alas, in spite of this situation being indisputable, we yet again find lobbyists like Willox calling for the government to resurrect those failed schemes.
But Willox is so concerned about the decline in building, if immigration is not increased, talking of:
“[…]The huge implications for many industries, particularly housing and construction.”
And it is the housing/construction sector interests that expose precisely what the whole Big Australia agenda is built upon. Excessive numbers of highly compliant immigrants will fall for the con-trick of borrowing big sums of money to buy a property. This will sustain the huge Ponzi-scheme.
Australia is now wallowing in crisis but those with the money are pushing for a new round of lunacy in furthering the disaster dumped upon Australians.
The extension of State of Emergency in the other five states does not need legislation, unlike Victoria. Here's information on the relevant laws for comparison, plus actions taken under similar legislation for COVID-19 in states outside Victoria. We have also now received a Report to Parliament on States of emergency - jurisdictional comparison, which shows clearly what the Victorian Premier is up against.
WA s56 Emergency Management Act 2005
2) The Minister must not make a declaration under this section unless the Minister —
(a) has considered the advice of the State Emergency Coordinator; and
(b) is satisfied that an emergency has occurred, is occurring or is imminent; and
(c) is satisfied that extraordinary measures are required to prevent or minimise —
(i) loss of life, prejudice to the safety, or harm to the health, of persons or animals; or
(ii) destruction of, or damage to, property; or
(iii) destruction of, or damage to, any part of the environment.
(4) The making of a state of emergency declaration does not prevent the making of further state of emergency declarations in relation to the same or a different emergency.
South Australia Public Health Act 2011
87—Public health emergencies
(1) If it appears to the Chief Executive that an emergency has occurred, is occurring or is about to occur, the Chief Executive may, with the approval of the Minister, declare the emergency to be a public health emergency (whether or not the emergency has previously been declared to be a public health incident under section 86). (
2) A declaration under this section— (a) must be in writing and published in a manner and form determined by the Minister; and (b) remains in force for a period specified in the declaration (which must not exceed 14 days) and for such further periods (which may be of any length) as may be approved by the Governor. (3) The Chief Executive may, at any time, revoke a declaration under this section.
TASMANIA: Emergency Management Act 2006
s42
(3) A declaration of a state of emergency may not be made so as to have effect –
(a) for a period exceeding 12 weeks in the case of an emergency relating to disease in humans or animals; or
(b) for a period exceeding 2 weeks in any other case.
(4) The Premier may extend a declaration of a state of emergency for one or more further periods, each of which does not exceed the relevant period specified in subsection (3) , if satisfied that there are reasonable grounds to do so.
(5) The Premier may amend or revoke a declaration of a state of emergency at any time.
Different states use different terminology
WA
On 20 August the State of Emergency was extended to September 3
SA
On 22 August, the State of Emergency was extended for 28 days
NSW - Public Health Emergency in Place
To deal with the public health risk of COVID-19 and its possible consequences, the Minister for Health and Medical Research has made a number of Orders, under section 7 of the Public Health Act 2010.
The Public Health (COVID-19 Restrictions on Gathering and Movement) Order (No 4) 2020 contains directions on gatherings, the use of non-residential and residential premises and community sporting activities. The Order lists premises requiring a COVID-19 safety plan . Generally the number of people allowed on premises will be determined by the ‘one person per 4 square metre rule’. Limits apply to weddings and funerals on residential premises.
People can participate in outdoor public gatherings of not more than 20 people. There is a 20 person limit on visitors to a home. The Order directs employers to allow employees to work from home if this is reasonably practical. The Order commenced on 1 July 2020.
TAS
On 8th of July the State of Emergency was extended to 31 August
QLD
Public Health Emergency extended to 2 October - The Public Health Act 2005 (Qld) does not provide for the declaration of a state of emergency in response to a public health emergency, however emergency measures may be enacted following a public health emergency declaration.
Dan Andrews’ attempt to extend Victoria’s State of Emergency in order to manage COVID-19 has been portrayed by some in parliament as a power grab and as an attack on human rights. But Victoria is the only state in Australia where you have to apply to parliament to extend the state of emergency. Enforcing laws about masks, geographical limits to movement, and curfews could not be done under normal health legislation. That is why, without a state of emergency, State Premiers only ask people to take these precautions. We have obtained information about laws in other states and their history of using these for COVID-19, which you can read at "Law & history on State of Emergency other five states - COVID-19 & Andrews stouch".
According to The Age:
"The Premier has said an extension would also bring Victoria into line with other states. “Other states are able to extend and extend and extend further. They don’t have any limits. We, under these arrangements, will simply continue the existing set of tools, if you like.”
Each state and territory has different periods of time that a state of emergency can operate for but no limits on how many times it can be extended." (The Age, What is the state of emergency and why is there controversy over extending it?)
For me, Dan Andrews' explanation of why he is seeking to extend Victoria's state of emergency seems reasonable, in light of the grave threat I see in COVID-19. I have assumed that enforcing laws about masks, geographical limits to movement, and curfews could not be done under normal health legislation. That that is why, without a state of emergency, State Premiers only ask people to take these precautions. We have obtained information about laws in other states and their history of using these for COVID-19, which you can read at "Law & history on State of Emergency other five states - COVID-19 & Andrews stouch"
The perspective of a power-grab conspiracy has received a lot of media coverage and fits into a big-business, ‘conservative’ or ‘right-wing’ view that the dangers of COVID-19 are vastly overestimated. Obviously that also suits their immediate bottom-line.
To be convincing, they would have to prove that there really is no virus, no related chronic health impairment, no cascade of hospital admissions, infected staff, or deaths, to logically persuade that a state of emergency was purely a grab for power, in the presence of a world-wide conspiracy to hoodwink the public.
In the absence of a convincing argument, it would remain that, although a state of emergency prolongation might conceal a naked grab for power, in the circumstances, in Victoria, it seems to have an infection control basis. And we will find that all the other states will be happy for any measures to contain Victorian contagion. And we cannot blame them.
The ‘conservative’ power-grab accusation also partly dovetails into a more ‘progressive’ legalistic human-rights point of view about freedom denied. This view, while sometimes conceding that the virus may be quite dangerous, nonetheless insists that it can be dealt with in a softer way, that people can be trusted to wash their hands, wear masks and keep social distance.
This perspective has been proved wrong, however, in the state in question. Victoria has had widespread community sourced infection, most of it where the source has not been tracked down, and these infections only started to decline after Stage 4 lockdown.
Lockdowns are the only effective way to pinpoint and freeze infection sources. You can lock down activity to 5km, as Victoria has done, then follow it up by contact and genome tracing. It is impossible to follow up large dispersed outbreaks via contact tracing and genetic linage. They spread too quickly and widely.
Although 'most' (we don't really know how many) may abide by recommendations, it only takes one (and there are many more as we see by the number of infringements) to spread a highly infectious disease. Industry will and does flout every safety-regulation and law and so we need powers to prevent that.
That leaves the problem that if the demands for ‘freedom’ were granted, that would take away the rights of people who want strong infection control, which cannot be achieved without state administration.
New South Wales and all other states closed their borders to Victoria, but then New South Wales acquired infection from Victoria, where a severe outbreak erupted. After that, other states closed their borders to New South Wales. Now there is an outbreak in Queensland. West Australia, Tasmania, and South Australia, are COVID-19 free, due to maintaining hard borders against the other states.
In the arguments against extension of state emergency powers of lockdown about human rights to freedom or the power-grab scenario, are Western Australians, Tasmanians, and South Australians, enslaved? They maintain restrictions on freedom of movement in order to protect their populations and their populations want this to continue, because – it protects them! Other states want Victoria to maintain lockdowns for as long as is needed.
There is nothing free about being stalked by a virus. Lockdown is a result of the virus, not politics.
We have to choose our battles. If we let the virus infect the bulk of the population, and remain among us, we would have a long term lowering of life expectancy and much suffering, with quite a lot of immediate death, and our hospital system would suffer long-term. Several things would contribute to lowering of general life expectancy: One would be the increased vulnerability to any illness among people who have suffered chronic damage, particularly to heart and lungs, from COVID-19. Those people can have had apparently mild forms of the illness. (See German study finds heart inflammation in large percentage of mild COVID-19 cases.) Another would be that, if more young people became infected, a larger proportion of them would die or be long-term affected. The fact that it seems true that you can get COVID-19 more than once, and get sicker each time, increases the potential severity of the problem. Risk would also increase due to people moving up into the aging cohorts, thus becoming more vulnerable to COVID-19. Hospitals would become centres of infection, rather than beneficial, their knowledge base and function would deplete as staff succumbed to death, chronic illness, and fear. Their services would no longer be available to surgical and medical cases unrelated to COVID-19.
The girls needed a break. The university term had just finished and so had "lock-down". Students, Isla and her two housemates, Chloe and Emily, were anxious to escape Melbourne. Emily's friend Olivia who was studying at Adelaide University had been trying, for more than a year, to entice Emily over for a visit, and this seemed the opportunity. Of course all three girls would go over together and, as they all yearned for a seaside experience, after spending so much time in their rented inner suburban house, they booked into an apartment for five nights in Glenelg, not far from Emily. It would be great! They could go for walks along the beach every morning!
It was a very dull, cold, day when they left for Adelaide. They all felt both relaxed and excited. It had been a long term of study, and the first lock-down had been very stressful. University social life had been virtually non-existent since before Easter, with "social distancing", and then, for Isla, episodes of self-isolation, when travelling from Melbourne to her family in Hobart and back.
It was marvellous to get away and be on the open road! It felt almost as though normality was settling over the pandemic-stricken state. They stopped in Ballarat for a coffee, not sitting down in the cafe, as they would normally have done, but taking their drinks in disposable cups, each with a treat from the bakery, to a nearby park. Isla was in high spirits and, as the apricot filling of her danish pastry registered on her taste buds, she had an allover feeling that things would be OK.
They arrived in Adelaide the same day, just on sunset. Their GPS took them through the now lit up streets of Adelaide, to their accommodation in Glenelg. The accommodation was somewhat bizarre, in that it looked quite conventional as part of an old but well maintained brick house, but there was only one rather minimal sofa and low rafters in various inconvenient places, so they had to bend over to make their way from the living room to the kitchen and to their bedrooms. The establishment was run by an elderly couple who had a ten year old daughter. Unsolicited, the woman, who was probably in her mid sixties, gave them a long explanation of her in vitro fertilisation (IVF) treatment at an advanced age, resulting in a degree of fame and a much yearned-for daughter. She even showed them an ancient magazine featuring an article about this event! After such a long drive, the girls actually longed to unpack and relax, so were grateful when Samantha finally said good night, leaving six slices of bread for their morning toast.
That first evening, the girls took it in turns to lie on the sofa in front of the television, with legs dangling over the edge. The other two lay on the floor, on sleeping bags they had brought, in case they needed to sleep in the car. Such is the lottery of booking accomodation on the Internet!
The next morning they met Olivia, a third-year architecture student who, it was clear, had very much missed her former Bendigo school mate, Emily
In Adelaide it was possible to do far more than one could in Melbourne, where galleries, theatres, cinemas, and many restaurants, were closed, but in Adelaide there was some theatre and they took the opportunity of seeing The Book of Mormon as well as visiting wineries and galleries.
They had not been taking much notice of the news, as they were on holiday, and did not want the be continually brought back to reality. One day, though, their leisurely breakfast was interrupted by a knock on the door. It was Samantha, with her daughter Ellen by her side. Samantha was prone to histrionics and, in overly dramatic terms, conveyed to the girls that Melbourne was going into a second lock-down! The girls greeted this news almost with amusement, but Samantha was frantic. She was under the illusion that the girls had to return to Melbourne before it was locked down, or they would not be able to return at all! Isla reassured Samantha that they had the situation in hand and would still probably be leaving on the allocated day.
After Samantha and Ellen left, the girls started making plans. This lock-down did change things, but they knew they were not locked out of Melbourne. In fact, this was their opportunity to escape being locked in!
Did anyone want to return to Melbourne? Definitely not! Isla decided on the spot to return to Hobart and continue the next term of her course online, until Melbourne was unlocked. After all, she would be doing the course online, anyway, if she were in Melbourne. The year had been so disrupted, with cancelled placements and very few physical meetings with her fellow students and lecturers. She went online and booked a flight from Adelaide to Hobart, on the day they would have returned to Melbourne. Emily would return to Bendigo and Chloe would return to Shepparton. They had come over in Emily's car and Emily would drive Chloe home to Shepparton, before returning home.
They made the most of their last few days in Adelaide. On the day of their departure, Emily drove Isla to the airport, and then continued with Chloe back to Victoria. The parting at the airport was quite emotional, as none of them knew when they would return to the house that, together, they had called home all year.
Isla had a three hour wait for her flight, but once she was in the departure lounge, she relaxed with a course-related book she happened to have brought with her on important minerals in root vegetables. Her phone was charged so she was entertained. Two hours after takeoff, Isla was collecting her luggage from the carousel at Hobart Airport. Her sister, Bea, was waiting for her, and she was overcome with relief She had not realised how stressed she had been over the past few months, but now she was back to normality. It was was as though she had come from a different country!
They pulled into the driveway of their suburban Hobart home, overlooking the Derwent River. As one of her relatives once said, "You don't live in Hobart unless it's in a house with a view!" This had seemed a terribly privileged and amusing thing to say at the time, but now she appreciated the somewhat isolated privilege enjoyed by Tasmanians. She raced inside to be greeted enthusiastically by Terence the sheepdog. They both rolled on the carpet in delight at seeing one another. She and Bea debriefed for the rest of the afternoon until their mother, Kate came home from work.
The rules in Tasmania for a person returning from interstate were self-isolation for 2 weeks. Isla was resigned to this, and she did not really care, as she knew at the end of those two weeks, that she would be free. The Tasmanian Government had kept its population safe, and for this she was forever grateful.
When the two weeks were up, Isla stepped outside and headed towards the yacht club. Solitarily, she strolled along the beach. Never before had the water looked clearer, the sky such a pure blue, and the quiet of the morning enveloped her, at the same time seeming to give her space to expand her consciousness.
Epilogue:
This is Australia in 2020. The quality of life is different in each state and bad luck for you if you are in the wrong state. Isla was lucky to escape Victoria, as there are now few freedoms for its inhabitants, due to the Covid 19 virus raging through the state. Other states had all but eliminated the virus, but things went badly wrong in Victoria, and this has put other states in jeopardy. It will be a long time before the people of Victoria can actually fully occupy and enjoy their own state and their own country.
On Australian ABC's Q & A, 28 July 2020, "Fight of our lives," Bill Bowtell[1] alone seemed able to conceptualise the biological restructuring of our economic environment, although Gigi Foster, economist, NSW, seemed to know instinctively what she needed to combat in order to keep the global, privatised economy going. She advocated allowing people to die from COVID-19, Swedish-style, in order to maintain business more or less as usual. However, when it was put to her that this would make everything less predictable and also incapacitate our health-care system, with no end in sight for the virus, she could draw a logical conclusion, which was, "[...] If we keep our borders closed, until there is a vaccine, we have to restructure the industrial mix in Australia." But this conclusion, anathema to her ideology, seemed ridiculous to her.
Not so to Bill Bowtell, Adjunct Professor, UNSW and Strategic Health Policy Adviser, who has a history of success in policy-making and promotion in the HIV-AIDS pandemic. He said, "The greatest enemy here is nostalgia and looking backwards. The Australian economy, the 30 years of the boom, have gone. They have disappeared. They were the product of a plan that came in in the 1980s, the Hawke-Keating government and the subsequent reforms. That's gone. The assumptions that underlie that plan have evaporated. The globalisation, the international economy functioning as we used to know it. So now we need Plan 3. The third plan since the war. And that will take all of the intellectual capacity that we have in Australia, the committment of the Australian people - they've got to buy into it - and the economy that will be born now will be very different than the economy that we have been used to. We can do it. We can make a better economy. The question of borders - Look, in the world, the Coronavirus caseload is going up like a rocket. There will be no opening up of international borders, as people seem to think there will be. We saw, in the last few days in Europe, where they opened up the southern borders in Spain, and then they had to shut them down again, because, guess what, the virus kept going up. Now, we have problems also with the Australian borders. I cannot see the outlying states opening up to a situation where we have Coronavirus cases at the level we have in Victoria and New South Wales. I don't see Western Australia doing that. The Federal Government is in court at the moment trying to force the West Australian Government [to open (?) interruption by compere, saying time running out and gives opportunity to another panelist to make final comment.]"
Karen Soo, Executive Officer at the Haymarket Chamber of Commerce, said, "I think this is a time for universal pause enables us as a society to really review what's important, and I think, as all people, I think it's really created a lot of equity and parity. So, everybody's now looking at the homeless, it's looking at multicultural societies, it's looking at everybody to say, 'How do we work together? How do we move forward? And how do we ensure that everyone can have a future together? And I think, it's going to hopefully be - I am quite optimistic - I think it's an opportunity that businesses will review and innovate and work together - local communities will be very market-driven until the borders are open once we are safe enough to function in a new way. Like, there's going to be a new way to operate in business."
NOTES
"Bio:
Mr Bill Bowtell AO, Executive Director, Pacific Friends of the Global Fund. Bill is a strategic policy adviser, with particular interest in national and international health policy structures and reform. He trained as a diplomat, with postings in Portugal, Papua New Guinea and Zimbabwe. As senior adviser to the Australian health minister, Bill Bowtell played a significant role in the introduction of the Medicare health insurance system in 1984. He was an architect of Australia’s successful and well-regarded response to HIV/AIDS. Between 1994 and 1996, Bill Bowtell was senior political adviser to the Prime Minister of Australia. He maintains a close interest in the potential impact of the HIV/AIDS epidemic, and the other communicable diseases, on the social, economic and political development of the Asia-Pacific region. Since 2005, Bill was Director of the HIV/AIDS Project at the Lowy Institute for International Policy and, since 2009, the Executive Director of Pacific Friends of the Global Fund. Pacific Friends is funded by the Bill & Melinda Gates Foundation. In these positions, he has sought to increase knowledge and awareness of the challenges posed globally, and to the Pacific region, by the three diseases. He has written and broadcast extensively on these subjects and participated in many international and Australian conferences and seminars especially in relation to HIV/AIDS." Source: https://kirby.unsw.edu.au/event/kirby-seminar-mr-bill-bowtell-international-and-australian-perspectives-three-decades-hivaids.
It was a stifling summer night with the usual crowd at the jazz venue Jonathan had frequented regularly for the previous few years. On this particular night he was introduced to Ruth, a rather earnest, slim, dark haired lady, in her early thirties. Jonathan, although somewhat lonely following the recent acrimonious break-up of his marriage to Danielle, and consequent distancing from his young son David, was not seeking a new partner. He felt the need to sort out his feelings and his finances before taking steps in that direction. He and Danielle had sold the family home in North Caulfield, and now he had to find another house with only half the funds, while house prices were sky-rocketing. He really needed to get away by himself to think about his future.
Ruth edged her way from the other side of the table to where his group were seated and suddenly she was sitting next to him. A cold and distant manner came naturally to Jonathan and he found himself using it, despite her insistent, tipsy, approaches. He needed something stronger than beer, but resisted the urge. He felt danger and knew he had to remain sober. In any case, he had to drive home shortly.
As he got up to leave, Ruth jumped up, asking for a lift home. She grafted herself onto his left hand side, walking out with him and waving gaily to the others. Jonathan stiffly agreed to take Ruth home, even though it was out of his way. They passed the Temple Beth Israel synagogue, whereupon Ruth announced she was often part of the congregation there. Jonathan was silent, not wanting to reveal his habits. They arrived at her modest flat in Balaclava, where she almost insisted on a kiss goodnight and an exchange of addresses.
Jonathan felt fleeced by this overbearing woman, but consoled himself that he was not obliged to contact her, even though he had found himself saying that he would! Uneasily, he drove back to his serviced apartment in St. Kilda Road, opened his computer, and lost himself in esoteric electronic musical programs and exchanges with people in Seattle, Avignon, and Brighton, UK. Needless to say, although Jonathan did not contact Ruth, she was sending him SMSs before his head hit the pillow. By 9.00 a.m.the next day she had actually rung him, trying to persuade him to attend the synagogue with her that morning. She insisted, in fact, and Jonathan found himself standing in the lower hall of the Temple Beth Isreal Synagogue, witnessing a Bar Mitzvah of a child who was a complete stranger to him! He felt trapped, and wanted desperately to go home and finish the program he was writing for a musical score about the Holocaust.
His day, however, had been planned for him, and it finished beneath the orderly covers of Ruth's queen sized bed. Looking out the high window of her bedroom, he saw a brick wall, and knew he was in a new prison. Ruth saw him looking up, not sensing his sadness, nor caring really about how he might feel. She remarked how lovely it was to see something as neat as a wall of bricks with no irritating uncontrollable vegetation spoiling the perfection.
In due course, Jonathan bought a small house in a respectable area, next door to an almost identical house built at the same time some ninety years earlier. About a week after moving into the new house, he received a welcoming note of introduction from his next door neighbour, Carole, who had lived there for the previous twenty years.
About three weeks later, when Carole was gardening in the front, Jonathan, from the street, introduced himself and Ruth to Carole. After that and for the next decade, Jonathan kept to himself, and rarely spoke to Carole, or even glanced in her direction, if they were both outside. He once came to her front door to tell her he had been burgled and she, knowing it was a common occurrence, commiserated in a heartfelt way.
About a decade later, Carole noticed that Ruth was present next door a lot more and discussing "issues" with her as though she had taken over the job of attending to anything to do with Jonathan's house. Carole found Ruth rather unsettling as a personality. She would complain about something like too many cars in the narrow street and then she would couch this concern in terms of her global concern that nobody come to any harm. The concern became over-dramatised. Ruth gave the appearance of having befriended Carole, frequently discussing matters concerning the immediate environment. She was what one might once have called a busybody and a gossip.
Inside the small house, Jonathan hardly had a moment of peace. Ruth had moved in, and he knew that if they ever separated, he would lose half of this house, and his wealth would be effectively divided by four, from where it was before he and Danielle separated. He was worried that, ultimately, he would have little to leave his son, David. But it was too late. Ruth had taken over. She changed the decor of all the rooms, having everything painted a glaring white, covering the subtle pastels and dusty mid-tones that Jonathan had hardly noticed, but which he realised later had a soothing effect on him. Ruth moved his desk, so that he was sitting opposite his neighbour's window, facing straight into her lounge room. These windows, facing one another had until now been treated with the utmost respect by the inhabitants of both houses. Jonathan was uncomfortable, and always looked down, but this was the only place left for him to work, following Ruth's re-arrangements. Ruth was out of control, and he could do nothing about it.
Jonathan retreated from the situation, submerged in arcane electronic and theoretical musical propositions. He no longer knew what was going on outside this constructed virtual world he inhabited.
Ruth was not on medication and her need to order her environment increased with each control she put on the exterior and interior of the house. Jonathan became almost an irrelevance to her. She enclosed the back yard with high fences, and an inordinate amount of wooden lattice on top on two sides. The next task was to block out their neighbour to the south, Carole.
At a dinner party one night, where the conversation centred around property values and activities conducive to increasing the value of the domicile, a young lawyer mentioned the shade cloth method of forcing a neighbour to one's will, with respect to fences. He explained to Ruth and the other enthralled dinner guests, that if one attached shade cloth on top of the existing fence, then the fence height was extended legally by this measure. This would leave the neighbour with no choice but to agree to whatever you want, and to be henceforth in fear of this being done again and again, to any height. The neighbour would be powerless to do anything. Ruth was overjoyed, as this was free legal advice, and she could establish to Carole that she knew her rights, and Carole would be powerless.
Ruth got onto her task right away, bringing in a tradesman to erect half a metre of dark green shade cloth on top of the fence between the two houses. Carole came home from bowls one day, to find that there was a dark green band across all her treasured north-facing leadlight windows. Sunlight had been blocked! This also affected her sunroom a little further away from the fence, with an artificial green glow visible behind her plants. The dappled light and shadows of the varied foliage by the fence had been obliterated.
All Ruth had to do now was to wait for Carole to capitulate and beg her for a high fence and another metre of trellis on top. After all Carole was on her own with no obvious male support, and she would never be able to stand up to this. The council would never intervene, Ruth mused.
Several weeks passed. Carole was mystified about this acton on the part of her neighbour, and made many despairing but fruitless calls to the local council. She had to steel herself each time she made an approach, as the information she gleaned was minimal, and she remained confused and ignorant as to her legal rights. She was certain of her moral rights, but her neighbour seemed equally certain of her legal rights, asserting that she could do what she wanted on her side of the fence! She also told Carole to "go away," when Carole tried to ascertain what was going on.
One day Ruth was patrolling the tiny perimeter of her domain when she saw an errant twig with two leaves and a perfect, very pale camellia, smiling at her over the bottle green shade cloth, just out of reach. She marched to the shed for her secateurs and a ladder. Normally she would throw any of Carole's leaves and branches back over the fence for Carole to dispose of. This time though, she decided to put this specimen in a vase. She climbed up on the rickety ladder but still could not quite reach. Rather unsteadily, she put one foot up on the next rung and reached towards the intruder. The ladder rocked back and forth a few times, and then crashed to the ground with Ruth aboard. Ruth was aware of a chiily breeze seemingly in her mouth. She put her hand to her face and saw that it was covered in blood. She had caught her cheek on a nail protruding from the stake that held up part of the shade cloth! She screamed but her voice did not sound like her.
Next door, Carole turned off the vacuum cleaner, as she finished her lounge room. She became aware of the noise from next door. She did not dare go near the fence but she went outside. The screaming and crying were much louder now. She could not see over the shade cloth without a ladder so she raced back through her house to her neighbours' front door.
Jonathan answered the door after less than half a minute. "Something has happened in your back yard. I can hear screaming. You need to investigate!" Jonathan thanked her and raced to the the back door. He had been listening with headphones to a version of his latest composition called "Covid Nineteen, where had you been?" and had been completely absorbed for at least two hours.
He looked around the garden and, there to his left, he saw the ladder lying horizontal, with Ruth's legs tangled in its rungs. Blood was pouring from her face. There was a huge cut right through her left cheek, through which he could see her teeth, as the flap of her cheek folded open.
Jonathan called an ambulance. He couldn't imagine being able to drive, with Ruth in this state sitting next to him in the car and, besides, he wanted to get back to his composition
After Ruth had woken up from her emergency plastic surgery, Jonathan arrived at the hospital. In his hand was a solitary pink camellia in a plastic bag.
Ruth had bandages covering most of her head and all of the left side of her face. She was in significant pain. Jonathan did not stay long but left the camellia by her bedside in a small vase supplied by a friendly woman in a blue uniform.
Ruth was discharged from hospital after three days, but still with her bandages. Her first check up with the surgeon was two weeks later, when she was allowed to see her face. To her horror, her left side was not at all like the right side, and she looked very asymmetrical. There was a large purple scar cutting diagonally across her left cheek and the whole area was swollen with a crimson hue. The nurses changed her dressings and a further appointment was made for three weeks time.
Back home, Jonathan seemed even more remote than before. All Ruth seemed to talk about was her scar, for which she blamed Carole, for having an inconsiderate tree that grew towards the light, in defiance of her shade cloth boundary. Jonathan didn't quite get this logic, and shrugged as he shuffled back to his office to review his composition.
Three months later, Ruth's scar had healed but her face was still noticeably lop sided. The surgeon said that at the the twelve month mark what she would see would probably be the best that her face would ever be. Ruth could go out, but she was grateful for the compulsory face mask dictum from the government to slow the spread of the virus raging in her city. Jonathan and Ruth could not visit friends and nor could they have anyone over. These were the rules. Jonathan felt irritated with Ruth. "She used to put her energies into making fences and blocking out neighbours, but now she comes to me all the time for reassurance about her face. I need a rest," he sighed.
One day, later that year, Carole saw a moving van outside Jonathan and Ruth's house. Carole was surprised as she had not known the house was on the market. By the end of that day, Carole had a new neighbour, Beth, and that is another story!
Carole had heard nothing from Ruth and Jonathan from the time she rang their doorbell to let Jonathan know of what turned out to be Ruth's plight.
One crisp morning a few weeks after Jonathan and Ruth moved, Carole, a masked, rather frail figure, emerged from the front gate for a walk, in the tiny quota of winter sun before a hailstorm expected later that day. Her neighbour on the other side of Ruth and Jonathan's house greeted her in a cloth-y voice through a Donald Duck face mask. Jane told Carole that Ruth and Jonathan had separated after "the accident", and Jonathan had to sell up in order to pay Ruth out her share of the house, and that she and her husband were in the process of negotiating with Beth, the removal of the trellis extension of their boundary fence.
Carole felt a lightness and something almost akin, as she remembered, to happiness. The neighbours' properties would now be free of barriers blocking their views to the sky. This was a kind of freedom, so welcome after many months of the pandemic restrictions weighing on them so heavily, and looming over the minutiae of every ordinary daily activity!
Early this year, as the COVID-19 virus gained a toehold in Australia, the message from governments, via the media, was that the aim was to "flatten the curve" so that case numbers would be such that our hospital systems would not be overwhelmed. It was not to eliminate the virus altogether.
Why would governments not want to flatten the curve right down to the x axis and eliminate the virus from our population?
After the first National Cabinet of Premiers and the Prime Minister in mid March this year, the State Premiers, it seemed, comprehended the danger of the virus to their populations and immediately acted to protect them by introducing lock-down measures to prevent the spread of the virus.
Tasmania and the Australian mainland are both islands!
Tasmania locked its sea border by not allowing people in from the mainland without quarantine. The conversation on the ABC was that Tasmania was lucky, as it is an island. My immediate thought was that the mainland of Australia is also an island! We have a chance here to stop this virus in its tracks, and safeguard our population - all 25. 5 million of them!
But it was never the aim of governments to eliminate this virus, newly introduced to our shores. They had to protect the economy and say the appropriate things to be reported in the media. Eliminating the virus would mean an inconvenient slowing down or stopping of migration long-term, with off-putting lengthy quarantine measures, which would dissuade any overseas tourism at all. Imagine if all overseas skilled workers (previously arriving in their hundreds of thousands) had to self isolate in hotels for two weeks before starting work. Who would pay for this? It would actually be economically irrational!
Governments opting to risk people for Big Business?
Instead, governments have opted to run the risk of continuous virus outbreaks, and second and third waves, in order to appease the voracious appetites of Big Business. This is not stated overtly, but when a leader waves a white flag and says that elimination is not possible in a country, which this time last year was completely free of this virus, then it seems clear to me that their hands are tied. Note that Tasmania has not had a new case of COVID-19 for over 60 days. In other words, it seems that elimination is possible, and that this has been demonstrated.
Using the island principle within Australia: West Australia and Queensland
The Premier of Western Australia closed the WA border to the rest of the country and so that it behaved like an island. This has worked. Cases of COVID-19 there are now only present in returning citizens in quarantine. Queensland's border was closed to all other states, which has ensured the health of that population. It has also earned Queensland the honour and responsibility of becoming home to, and host of, Melbourne AFL football teams and their families. This will be quite good for their economy, as the Queensland government salivates over the possibility of hosting the AFL grand final, an event previously firmly associated with the Melbourne's MCG.
With Victoria in a parlous state of lock-down, grappling with increasing numbers of COVID-19 cases every day, this football history-making break with tradition seems very likely to happen for that very reason.
Why is Victoria different?
Victoria is the basket-case in all this - but why? At the beginning, the Premier sent largely the right messages, with respect to the severity of the situation, as we went into the first lockdown. I was surprised and pleased that he seemed to get it and to give it the priority it deserved. The first lock-down was put in place. For many weeks, unless people lived in the same house, or could meet outside at a distance, they did not see their friends and families. Every night on the ABC, we would see grand parents and grand children greeting one another via this medium, highlighting the sadness felt and the sacrifices made. Childhood is fleeting, as is old age, and the lost times together cannot be regained. This is only one example of the broken ties that the first lockdown entailed.
But it did not work in controlling the virus in Victoria.
How did Victoria become the basket case?
Eventually, the first lock-down eased and Victorians regained a degree of normality and freedom. Last month we Victorians could visit one another, as long as there were no more than five people in the one house. I dined one night with three other people, in a friend's house. Our places at the large table were judiciously distanced, but it was pleasantly reminiscent of pre-COVID times.
Unfortunately this relaxation of isolation was short-lived. In recent weeks, increasing numbers of new cases of COVID-19 were being identified in Melbourne, and it came to light that there had been breaches of the hotel quarantine system for people returning from overseas. This debacle is the subject of an enquiry, but rumours abound of security guards getting into bed with the returnees, ad hoc staffing with SMS messages to friends, offering them a gig at a hotel, guards "moonlighting" and doing two jobs at once (actually absent from their posts.) Although these are rumours, it is clear that this important job was not taken seriously by those who organised it, by those assigned the task, nor by the returnees, who had they any respect for their fellow citizens, would have acted in a more trustworthy manner.
As a result of this and other breaches, including reported large family celebrations, Victoria now has a daily rising number of cases. Yesterday, July 17th, 425 new cases were reported, and Melbourne is back in lockdown, the rules of which are somewhat vague around the edges, with punitive fines seemingly at the discretion of police.
Still not aiming at eliminating the virus from Australia
Yet we are still not aiming at eliminating the virus in our population. If Victorians knew that the aim was to eliminate the virus from the population, it might maintain their motivation. It could also be successful but a series of relapses, accompanied by disturbing news of our hospitals struggling to cope, is ultra dispiriting. If our health system collapses what do we have?
Australia must adopt an elimination strategy for COVID-19
Australia must adopt an elimination strategy and send this message clearly to its population. if we don't eliminate COVID-19, we will never be free again. We have a large, beautiful country, but we can't move around in it. Soon, in Melbourne, we may not be able to move from our own post code. This would be bearable if we knew we were aiming to be free again but, at present, all we can see, is a recurring and chronic situation of restrictions, which are eased and then reimposed, but never lifted.
This video is from Dr Mike Hansen's excellent medical channel, June 16, 2020. Dr Hansen works in Emergency Medicine as a pulmonary specialist and has made a number of highly informative videos on the subject of covid 19.
Transcript for the above video, originally entitled, "Does Blood Type Matter for Coronavirus (COVID-19)?."
People have either blood type A, B, AB, or O.
Are people with blood type O less prone to suffer from COVID-19? And does blood type A make people more prone to COVID-19?
Let me first start out by saying that people of all blood types can get COVID. And people with all blood types can possibly die of COVID if they get the infection.
But, based on several different studies, it looks like people with blood type O have less a chance of getting COVID-19, and people with type A might have a higher chance of getting the infection.
Data from China was the first to show the ABO blood group association with COVID-19 infections.
The researcher Zhao and others compared ABO blood groups of controls from the general population with over 2100 COVID patients from three hospitals in Wuhan.
Across all three hospitals, blood group A was associated with a higher risk for COVID compared with non-A blood groups, whereas blood group O was associated with a significantly lower risk for infection compared with non-O blood groups.
There was another observational study on data from the New York-Presbyterian hospital system, which happens to be where I did my fellowship training. So there, over 1500 people tested for COVID, and they had similar results with blood types.
There was another study done by Andre Franke in Italy and Spain.
In this study, they looked at DNA samples from 1,980 COVID-19 patients who were hospitalized for respiratory failure. And the study produced similar results.
But what about the severity of illness?
Does having blood type O, make someone less likely to have a severe illness from COVID, compared to type B, type AB, and type A?
Well, Zhao and others looked at the case fatality rate, and blood group A was linked to higher mortality risk compared to blood group O.
Interestingly, the association of blood type is not explainable by other risk factors, like obesity, diabetes, and high blood pressure.
Recently, there was a study published by the personal genetics company 23andMe regarding evidence that blood type plays a role in COVID-19.
So if you don’t know, 23andMe is a company that sends out personal genetics testing kits to individuals who are interested in finding out their genetic history and or their predisposition to certain genetically transmitted diseases.
According to their website, they did a study based on over 750,000 people.
Their preliminary results suggest that O blood type appears to be slightly less susceptible to contracting the virus.
But the big question is why?
No one really knows, but there are a lot of hypotheses.
BLOOD TYPE is determined by genetics, and the genes determine the specific proteins on the surface of the cell. These proteins, then have specific sugar molecules that are added to them. They exist in our blood cells and other cell types.
People who are blood type A carry A-sugar-antigens
People who are blood type B carry B-sugar-antigens
People with O blood type have neither A nor B-sugar antigens.
What is the significance of this?
This means that the immune systems of people with type A blood develop antibodies for B antigens.
People with type B blood type have antibodies for A antigens.
People with type O blood have antibodies for both A and B antigens.
People with AB blood type will have neither anti-A nor anti-B antibodies.
And here is an interesting fact we knew before COVID.
There are studies showing that people with type O blood have lower levels of proteins that promote blood clotting.
More specifically, people with blood group O have about 25% lower levels of von Willebrand factor (VWF) than those with types A, B, or AB. This is due to increased clearance of VWF from the circulation.
VWF is always involved in the development of clots, so if there is less VWF, there’s likely to be less clotting. So this might explain why Type O blood type means fewer blood clots, and this might at least partially explain why people with Type O overall have less severe disease. Because as you probably know already, lots of people with COVID pneumonia also have blood clots. Also, we know that the SARS-CoV-2 can replicate in cells that express blood type antigens. Such as the cells that form the lining of our lungs, and the cells that form our tiny little air sacs, the alveoli. And the cells that line the inside of our mouth and nasal passageways. This means that when an infected person coughs or sneezes, there's a possibility that they release viral particles that are coated with their blood type antigens. So this is at least a theory from some scientists.
In Melbourne last Saturday nine public housing towers with 3,000 residents were shut down for at least five days, due to a large cluster of identified cases of COVID-19 within their walls. Since then, of course, the whole of Melbourne has been locked down for about six weeks. And this is a Melbourne burgeoning with high-rises. It seems a lifetime ago, but it is only about five months since the cruise ship, Diamond Princess, with identified cases of COVID-19 was unable to disembark in Yokohama, Japan. Her hapless passengers were confined to their cabins, in an attempt to prevent the spread of the virus aboard the ship and on land. Predictably however, the virus spread through the ship and by early March there were six casualties.
Those of us who see the downside of "storing" people in high-rise buildings and advocate against this trend in Australia, immediately saw high rise towers as vertical cruise ships. This obvious comparison has become a widespread notion, and many of us are trembling observers of this latest selective lock-down of the towers in North Melbourne and Flemington.
It is difficult to conceive of what the Victorian Government could have done differently in the situation and constructive criticism is equally difficult.
It is, however, easy to criticise the rapid trend towards increasing living density, both in Australian cities, and in most of the world. Beginning with the extreme: high rise, such as the public housing tower blocks, which have been there for many decades, but are being replicated in form all over our cities - this is not a sustainable way of living for humans. It is suitable for a few nights in a hotel when visiting a large capital city, but as a long term arrangement it is anathema to what most humans need. People may choose to live in an apartment out of economic necessity. In some cases, apartment-living may be seen as convenient and labour efficient for the resident, not requiring maintenance of gardens and fences, for instance. It is also secure for those who travel a lot. These reasons make sense for the solo person making his/her way, in a globalised business world, for example, but for those less peripatetic in their work habits, the advantages over a house and garden are dubious.
The COVID-19 crisis has, over the last few months,brought the problems of apartment-living into sharp focus, particularly with this latest lock-down.
COVID-19 has thrown us all back on our own resources in 2020, and those with more resources have suffered less. People who have gardens are in a better position than those who do not, because they can be outside, yet remain safe from infection by others. At present, people in Victoria, including people in apartments, cannot easily travel outside that state. Many of us are yearning to exchange winter in Melbourne for two weeks near the beach in Queensland, or even the milder climate of southern New South Wales, options that were so available to us before the current health crisis. But these are minor frustrations compared with the constraints under which the residents of the public housing towers are being held right now.
For years, some of us have seen the undesirability of normalising high-rise living in Australia's large cities, and we noted the helplessness of people in towers in the face of dangers like flammable cladding, or major plumbing issues that required evacuation. This is not to say that a house cannot catch fire or flood due to a plumbing problem, but the impacts of such crises are massively multiplied in towers with hundreds of residents, where the effects of being locked in or out are very serious. Residents in towers are at the mercy of the buildings' private or government owners. The high rise arrangement may be workable when all the complex functions of a large city are operational, but this cannot be guaranteed.
Population growth, engineered by governments and planners, is hypocritically given by them as an excuse for the transition in Australia's capital cities, especially Melbourne and Sydney, to ever increasing density. Increased population within a given area does not serve us well. It advantages those who make money from high volume sales - from the sandwich bar near a block of offices, with an imperative to meet its high rent, to those who own our toll roads and transport systems. Surely, we, as a society, have to admit defeat with respect to the notion of ongoing high volume being the commercial panacea for all transactions? We cannot "socially distance" in a crowded restaurant, in a capacity crowd at a football stadium, cinema, orchestral concert, ballet or theatre. Fortunately for the toll road owners, heavy traffic is not an immediate COVID-19 health risk, but if our roads are the only place we can now gather then one might hesitate to call the resulting human accumulation in cities any sort of society.
The problems encountered in tower blocks in recent years are the indicators that we have hit the wall with respect to density of human habitation. We have had several warnings with the current one being loud and clear. Wrong way! Go back, or at least go in a different direction!
The Victorian Government’s master planning document, Plan Melbourne— which drives high density development throughout our suburbs—assumes continuing rapid population growth over the next decade. The coronavirus pandemic, and the Federal response to it, means this assumption has been overtaken by events, and that Plan Melbourne is out of date. The Morrison Government expects a fall of up to 300,000 people moving to Australia over the next 2 years. The Federal Government expects net overseas migration to fall by 30% in the current financial year, and to crash by 85% in 2020-21 to around 40,000.
Some of the drivers of this fall are outside Australia’s control, such as lockdowns in other countries and a collapse in international air travel. However the Federal Labor Opposition has also signalled a reduction in migration, calling for Australia’s immigration to be overhauled and curtailed in the wake of the pandemic. Opposition
spokesperson, Senator Keneally, has written,
“Do we want migrants to return to Australia in the same numbers and in the same composition as before the crisis? The answer is no”.
Against this background, the Victorian Government needs to quickly reassess Plan Melbourne—which makes high rise and high density housing a planning priority at the cost of any other considerations. Otherwise we risk being caught living in the past. It is likely that businesses that have developed a dependence on rapid population growth will struggle, and the Victorian Government needs to plan for this.
It would also be wrong for the Government to continue to impose rules enforcing denser populations on communities that don’t want them. Plan Melbourne has been a vehicle for Councils to be told they have to accommodate “their share” of Melbourne’s population growth. The Government should revisit its population projections, and not be caught out by a potentially fast changing population landscape.
It certainly should not continue to impose high-rise coronavirus traps, forcing people to live on top of each other, on unwilling communities.
The evidence around the world is clear –a dense population is a vulnerable one. The Victorian Government needs to understand that the game has changed, and move with the times.
Daniel Ziffer's journalistic effort for the ABC Saturday May 9th, "Calls to cut immigration often ignore Australia's economic and social reality," was sparked off by Shadow Minister for Immigration and Home Affairs, Senator Kristina Keneally's week old article, calling for a review of the numbers of skilled temporary workers. The purpose of the review she was calling for was to give Australians who have lost their jobs due to coronavirus lock-down, first preference in the job market when "normality" returns. This mild and reasonable suggestion has met with a frenzy of opposing articles in the mainstream media, and this ABC concoction is yet another of these.
In summary, the article is making the points that our social reality is multi-ethnic, as indicated in a photograph; and that senator Keneally, because she is an immigrant, has no moral right to suggest lowering the numbers of skilled temporary overseas workers following the Covid 19 crisis. Ziffer wrote (in the article) that Australia's important money-earners include "opportunity and growth". He uses the example of a successful migrant who is making money from population growth, which in turn is meant to illustrate the need for ongoing immigration and population growth (!).
Ziffer also notes that GDP per capita is actually falling, wages are "stagnant", and that people feel they are going backwards. Yet he later says that "We've become vastly rich — economically as well as a society — because of our diverse make-up." (!) Which is it? Are we feeling left behind or are we vastly rich? Does it depend who we are?
His closing comments relate to his earlier criticism of Senator Keneally for having the temerity, as a migrant, to make a public statement on immigration settings, even though she is the Opposition spokesperson on Immigration and Home Affairs!
He finishes up lurching to the extreme of calling this, "closing the door" to immigration (which was not suggested by Ms Keneally nor any other published commentator in the news this week), saying this cannot be done, because it would mean all of us - apart from the just over 3% of us who are of Aboriginal or Torres Strait Islander heritage - would be denying our ancestors, since they were all migrants.
So, from the Ziffer perspective, Australia is locked into perpetual immigration, at a rate that cannot be questioned, by those who live here, those who come here, and even by the the Shadow Minster for Immigration and Home Affairs!
Will governments buy back vital resources and essential services from the embattled private sector, or will they allow the wealthy to pick up resources and monopolies cheaply, pressing the unemployed and endebted into slave-like conditions? Can we adapt to or avoid a future that appears to hold more and worse pandemics? If COVID-19 is a pandemic designed for elite purposes to cull the aged and weak, why have some governments tried to protect their vulnerable populations? We have obviously become too economically dependent on the model of continuous accelerated growth in human numbers and human activities globally to be able to protect ourselves from the pandemics that come with this economic model. At the same time the long-predicted oil-resources breakdown in supply is looming. Can any good come of this? Is this an opportunity?
There are many reasons why a return to normality after COVID-19 is unlikely.
The underlying reason is the world-trend to a rapidly increasing incidence of serious new cross-species viral diseases (zoonoses). The most likely to produce epidemics and pandemics are those coming from large populations of domestic animals raised in intensive farming. Where once a zoonose would probably kill a novel host before the virus got a chance to jump to another individual, our new tendency to put livestock together in vast dense populations, along with our increasing tendency to live in vast dense populations ourselves, means that viruses can find multiple hosts to replicate in before their first host dies. Because we have no specific immune defenses against new zoonose viruses, they are much more likely to infect and kill us than longstanding human diseases.
The embedded video below, Flu Factories, gives a graph between 1951 and 2006, showing that international progression of avian flus (among the most dangerous sources of zoonoses shared between pigs and birds), began building up with the institution of ever larger factory farms around the 1980s, and skyrocketed from the beginning of the 21st century.
It quotes a summary of the components of risk:
"- Increased demand for poultry products.-
- Increase in commercial peri-urban production.
- Increase in size of susceptible bird population in interface between extensive and intensive production.
- Increase in pathogenic virulence.
- Enhanced exposure in human population.
- Emergence of human pathogen.
- Human-to-human transmission pattern."
Dangerous divide between veterinary and human health sectors
Writing of the east in 2014, the World Health Organisation notes
"[The lack of] collaboration between the animal and human health sectors under the concept of “One Health” approach, which links the human with the animal health sector integrating the animal and human disease surveillance and response system that could, otherwise have helped controlling the zoonotic infections in animal reservoirs, enable early outbreak detection, and prevent deadly epidemics and pandemics." [Source: World Health Organisation: http://www.emro.who.int/fr/about-who/rc61/zoonotic-diseases.html [1]
This collaborative failure was and is also a major problem in the west, which, in the problem of COVID-19 control, amounts to a failure of communication in the context of dissimilar paradigms between the economic sector and the health sector. So, we have health professionals urging quarantine and business urging abandon of quarantine. We have obviously become too economically dependent on the model of continuous accelerated growth in human numbers and human activities globally to be able to protect ourselves from the pandemics that come with this economic model.
We could mitigate some of the risk within the current system
The above-cited World Health Organisation article http://www.emro.who.int/fr/about-who/rc61/zoonotic-diseases.html, which has a number of useful recommendations, correctly suggests that practising barrier nursing for all hospital patients would probably avoid almost all epidemics. Unfortunately, after antibiotics became widely available in the second half of the 20th century, hospitals all over the world became increasingly casual about infection control.
And we could return to reusable and locally produced hospital equipment: Post 1970s, with growing reliance on plastics and paper disposables, hospitals reduced their independent options by abandoning much in-house sterilisation of reusable instruments along with the laundering of reusable gowns, masks, and other protective equipment. As we know, the reliance on cheap imported sources for disposable equipment and tools has defined 21st century inadequacy in the management of COVID-19.
If we return to business as usual, however, with factory farming, clearing of wilderness, dense human populations, mass people movement internationally, and international trade, especially in animals and plants and their products, we will continue to experience pandemics. Some will have much higher fatality than COVID-19.
Politics of the current pandemic
The current pandemic is like a test of our social and political resilience, as well as our immune resilience, and its management presents something of an economic and moral puzzle, because of COVID-19's tendency to cull the weak and elderly - those people we have been taught by popular economic rationalism to blame all our woes on. (See /taxonomy/term/265 and /taxonomy/term/393.)
Whilst COVID-19 might look like a pandemic specially engineered on order from economic growth lobbyists who scapegoat the elderly and infirm, whilst encouraging mass migration of younger, haler, more fertile, cohorts, deemed economically more productive, this may only be coincidence.
Britain, Sweden and the United States have behaved more in tune with such economic ideologies, throwing their populations to the wolves, with cries of 'herd immunity'. Some governments, however, actually seem keen to avoid this opportunity of culling the elderly and infirm, when they have previously been so disparaging and cruel towards them. Australia and New Zealand are examples of such countries. What could explain this apparent humanity among an elite composed of economic rationalists, who generally only value their populace on condition of high productivity? Did politicians' wives, mothers, and fathers, get to them? Or is it because most at the top of government, political parties and corporations, and armies, are old themselves? Is it about the look of it, the desire to avoid mass graves and piles of cardboard coffins, US and Brazil-style? Is it about avoiding a glut of cheap housing and plunging property prices? Is it about avoiding total collapse of the hospital system, when surely they could have sequestered parts for themselves? Is it about avoiding economic collapse of old-age care businesses? Is it about currying favour with the elderly voter cohort? Is it about an exercise in preparing for the next worse epidemic? Is it about fear that the public will revolt at the prospect of their elders drowning in putrefacted lungs? Is it about shock at the prospect of shiny economic principles besmirched by medieval suffering and dirt?
It is certainly hard to figure out. Maybe what happened was that the pandemic took the mainstream press by surprise, and what we got, for a change, was a spontaneous response by the usually pre-programmed journalists. The elites, who are normally spoon-fed by the mainstream press, and protected from realising how angry some voters are, were panicked at the idea of popular rage. Usually they are protected from our perrenial rage at housing prices, homelessness, and rotten wars, because it is rarely reported and we have no independent public talking stick and means of assembly, so are unable to organise beyond indignation and that indignation is largely impotent because invisible to the political class. I take the near collapse of the anti-war movement as my model in this, since it appears to have been related to the mainstream press having simply stopped reporting on anti-war protests after the last big world protest against the Iraq war. Whilst I would like to believe that the alternative press can take care of reporting, it does seem that the mainstream still dictates the propaganda, hence what the elite politicians react to.
So, did politicians in Australia and New Zealand react to protect their vulnerable populations simply because they were afraid of public indignation? (All the while preaching against the use of protective face-masks.)
Or did the mainstream press jump at the opportunity to sow economic panic, so that media moguls and their friends could buy up assets and businesses cheap? And the politicians fell in with this plan under pressure to avoid public indignation about plague.
An engineered virus commissioned by elites?
There is little evidence to suggest that this virus was engineered, but a not insignificant number of people believe that elites would do so. After all, elites maintain massive military machines that design biological warfare, and constantly engineer the most brutal wars-for-profit in what has become the biggest game in town. But why would they or anyone need to commission a zoonose flu, when we have so many new zoonoses coming on board at faster and faster rates, from massive factory farms, and from the bush, as human population expands into what remains of forests and wildernesses, displacing exotic animals, and sucking the last endogamous and sedentary tribes into the vast human homogeneity hopper?
"During the past decades, many previously unknown human infectious diseases have emerged from animal reservoirs, from agents such as human immunodeficiency virus (HIV), Ebola virus, West Nile virus, Nipah virus and Hanta virus. In fact, more than three quarters of the human diseases that are new, emerging or re-emerging at the beginning of the 21st century are caused by pathogens originating from animals or from products of animal origin. A wide variety of animal species, domesticated, peridomesticated and wild, can act as reservoirs for these pathogens, which may be viruses, bacteria, parasites or prions. Considering the wide variety of animal species involved and the often complex natural history of the pathogens concerned, effective surveillance, prevention and control of zoonotic diseases pose a real
challenge to public health." [Source: "Report of the WHO/FAO/OIE joint consultation on emerging zoonotic diseases," (May 2005) p.5. https://apps.who.int/iris/bitstream/handle/10665/68899/WHO_CDS_CPE_ZFK_2004.9.pdf]
Why would elites encourage something that, anyway, threatens to put the kybosh on economic activity and mass people movement? Have they seen the writing on the wall, the collision of overpopulation with undersupply? Is this a way for them to lock populations down so they can control revolts against mass immigration? But the lock-downs stop mass immigration.
You could argue that big fish that survive will be able to buy up multiple businesses and assets dirt cheap, in the way that Mr Soros picks up currencies and coal mines cheaply in the wake of wars and climate activism. In the short-term, it would be hard to counter this one.
In the longer run, however, inevitably, more virulent viruses will have the effect of sparsening populations, ultimately making them less infective. Substantially sparser populations world-wide will really wreck the connective fibre of the international capitalist system, and will probably wreck national systems, sparing all but local systems. Depending on how much populations and global trade and travel are reduced, humans will spontaneously reorganise into small viscous populations, developing their own local immunities.
The elites, however, may well benefit from this too, on the way down. This would be because, if we spiral into depression, people will work for tiny wages, even for their keep, or as slaves, everywhere, creating local alternatives to both imported and outsourced cheap overseas labour.
Oil prices....
At the same time as the pandemic, the long-predicted oil-resources shortage is looming, although it is initially presenting as an oil-glut. Reduction in economic activity through mass quarantines has led to collapse in demand for petroleum. Since the 1970s, oil discovery and production have become increasingly difficult and costly. Easily drilled and pumped sources of crude have long given way to hard-to-access mixed liquids and gases, including fracked and vegetable ones. Oil exploration and production decline and stop in the absence of sufficient investment. Overleveraged companies fail under economic stress, especially with the kinds of costs involved in oil-exploration and exploitation. Countries dependent on oil-revenue descend into economic depression. Supply chains are disrupted by business failures. Machinery falls into disuse. Skills are lost or poached. Predators and competitors destroy oil-fields in order to privilege their own production recovery. Ultimately governments and conglomerates, including banks, will be able to buy up oil exploration and production cheap. Western governments have tended to enable corporations, to the detriment of economic and equitable supply, and have gone in with their war machines to destroy or wrest oil production from public companies in Iraq, Libya, Syria, Venezuela, etc. The stop and start mode is inherently costly and disruptive. Probably the only reliable mode of oil and gas production is by governments, which do not have to make a profit. As Colin Campbell wrote in the 1990s,
"The Soviets were very efficient explorers, as they were able to approach their task in a scientificmanner, being able to drill holes to gather critical information, whereas their Western counterparts had to pretend that every borehole had a good chance offinding oil." [Source: Colin Campbell, "The Caspian Chimera," Chapter 5, in Sheila Newman, Ed. The Final Energy Crisis, 2nd Ed., 2008]
Some possible solutions and adaptations
The COVID-19 pandemic has revealed fundamental weaknesses in global supply system.The need for governments to take over outsourced services and resources in order to provide for vital needs reveals the fallacy of privatisation for profit, and exposes the notion of privatisation for 'efficiency' as laughable.
The failure of private businesses and corporations provides a serendipitous opportunity for governments to cheaply buy back vital resources, such as land, power and water, and essential services, like airlines, roads, hospitals, land-production and housing etc.
Deglobalisation of the economy means ending mass migration and foreign ownership of resources and essential services.
Without Australia's massive population growth, which relies on mass immigration, the land and housing sector would no longer support our huge and immensely costly private property and infrastructure development industry. Until Primeminister Menzies in the 1960s, who also encouraged mass immigration, government was the main land and housing production source.
Governments now have the opportunity to re-regulate land and other vital resource prices in order to reduce the cost of living and production, to get us through the coming economic depression, and beyond. Lower land-prices would mean more local ownership and the opportunity for more local food production, proportionately reducing the need for the cash economy. These changes would make it possible to reduce the hours of work that people need to earn a living and the need for consumerism to support more workers.
Governments should also be able to organise the share of essential work more equitably.
Populations in lock-down have had the opportunity to investigate the notion of leisure, the meaning of life, and even to smell the roses. Released from the treadmill, but at risk of their lives, more may have started to question the authority of the elites and be more willing to participate in political self-determination. Nonsensical advice about not wearing masks, which must have had fatal consequences, was given by the highest authorities in the land. Will this lead to wider public loss of blind faith in media-created and promoted figureheads, resulting in ordinary people doing their own research and testing and trusting their own judgement, finding leaders locally, rather than accepting the leadership choices and policy dictates of a distant political caste?
NOTES
[1] This paper is undated but appears under the "Comité régional » Sixty-first session," which made its annual report in December 2014.
In this article, Sally Pepper proposes that there is an economy with a small 'e' and The Economy with a big 'E'. As well as threatening its survival, COVID-19 has called the big E economy into question. Sally says, "The economy with a small 'e’ is a way of describing what we do. The Economy with a capital “E” is something we serve, whether we like it or not. To please The Economy we have to behave in such a way that it looks its best and is pleased with itself. The Economy seems to be like a teenage boy, with a voracious appetite. It never develops beyond the need to grow bigger, endlessly. It is like a monster that we have given rise to and are doomed to cater to forever."
The corona virus has been really bad for “The Economy.” We can tell that from the falls in global stock markets over the past few weeks. Those whose wealth is in stocks are now poorer or at least not as rich. The stocks have fallen, mainly, I assume, because of smaller earnings, due to decreased activity and, therefore, anticipation of lower or no dividends for shareholders. There are of course winners and losers, but the indices are telling us clearly where the stock market has headed.
Air, land,and sea traffic, have all diminished, globally. Traffic within cities, towns regions, and countries, has also diminished, as people comply with lockdown requirements. This means that less fossil fuel is being burned, and so there are fewer emissions, and clearer skies have been noted in many cities of the world.
The kinetic aspect of humanity has been toned down. Movement has slowed. Less work is being done, at least less of the work that went into earning money. People are now working on projects at home that they have been postponing for years for lack of time. This transfer of effort is very bad for The Economy.
Shops, other than supermarkets, pharmacies, and other outlets for essential goods, are now closed. Restaurants, clubs , sporting facilities, and gyms, are now closed . Workers have been laid off, but the government has chipped in to provide a living income to those expected to return to their previous employment, when life returns to normal. I assume those employees are now catching up with cleaning the bathroom, weeding the garden, planting seasonal vegetables and having time to think………as I am
Immigration and travel have stopped. Foreign nationals and non-residents are not allowed into the country and returning nationals have to spend two weeks supervised in isolation in hotels before going to their place of residence, which is where we are all in various states of isolation. The frenetic pace of growth has slowed to a near standstill If this new state of affairs were to continue, it would mean a rest from construction and road works, and less destruction of trees and gardens in the urban areas of Victoria. We are, in fact, headed for that most dreaded economic state of affairs - a recession. This translates into a very sick Economy! Might The Economy even die?
We, however, will still go on living, as long as we escape the clutches of the virus.
What will life be like? We already have some idea, as we are now living it and have already started changing. We could, in future, turn our focus to more essential activities, like gardening and producing food, doing repairs around our homes to ensure they remain standing and weather-proof, and sewing masks to protect us from the virus. We might start to get creative in the community sense, growing and exchanging produce. We could get to know our neighbours, who we have been too busy to speak to hitherto. We could learn from the alternative fringe of future-focused urban farmers, tucked away in newly gentrified inner northern suburbs, or in the less fashionable outer suburbs of Melbourne, or in the nearby countryside. These re-born farmers are generous with their knowledge, which can also be found on sites such as Face Book and You Tube.
With the loss of jobs, many renters have been left in the position of not being able to pay the rent. This is a problem for the renter and the landlord, especially if the landlord is making payments to a bank. In normal times, with hundreds of thousands of people entering Australia every year, the landlords would have their choice of paying tenants, but with the human avalanche stopped in its tracks, the landlord might just have to negotiate with both his bank and the tenant, for a mutually agreed outcome, and as little stress as possible. As we are being told in the mainstream media, “We’re all in this together.”
It seems to me that even if things do not go back to normal we can work out a new way of operating – something we negotiate amongst ourselves.
But am I being inconsiderate of The Economy?
An economy, at its most fundamental, is the sum total of the commercial activity or exchanges that happen between us. In the absence of overarching forces, we will work it out, especially if we have to. Economic activity will not cease, but it will be fit for purpose. I would call this our "economy with a small ‘e’". This economy is not our monarch or our religion, and it is not something we must serve. Our society, behaving in our own best interests, creates this economy. The economy with a small 'e’ is a way of describing what we do. The Economy with a capital “E” is something we serve, whether we like it or not. To please The Economy we have to behave in such a way that it looks its best and is pleased with itself. The Economy seems to be like a teenage boy, with a voracious appetite. It never develops beyond the need to grow bigger, endlessly. It is like a monster that we have given rise to and are doomed to cater to forever.
Do we really need this demanding perennial teenager, The Economy? Or can we just get on with our lives and let it become a decent citizen and part of our community?
The deletion of the comment quoted below in this notification is perhaps the most odious of all those made under this article today, all done without any clearly discernible reason but with quite evident rhyme. The comment below asks you to show respect for these commentators who have suffered deletion of their genuine and reasonable comment by providing an open advice as to the basis of that consistent disbursement of negative action.
The unavoidable message from your early closure of comments, following directly upon the posting of the request for your reasoned advice, is that you do not have respect for your reader and commenters. It also clearly demonstrates your publication’s covert imposition of a controlled narrative rather than being the relatively free arena for informed adult conversation that your promotion pretends you to be.
As I’ve already made mention of, as the repetitive and unexplained evidence mounted, your pretence and hypocrisy as an intellectual forum is comical; sadly, bleakly, disturbingly so, but comical nonetheless.
With some good fortune the cumulative load of Covid19 distress will be the death of your horridly sneaky and cynical enterprise. Hopefully, well-meaning staff will then find some useful jobs in which to sustain themselves within a wider community in need of real re-construction that is free of the property development, migration agency and associated Empire roles that your sponsors pursue ahead of real education, with the active assistance of this mouthpiece.
Kindest regards
Greg Wood
On 14 Apr 2020, at 4:51 pm, The Conversation wrote:
The Conversation
Academic rigour, journalistic flair
Hello Greg,
Your comment on ‘Why is it so hard to stop COVID-19 misinformation spreading on social media?’ has been removed.
There are several reasons why this may have occurred:
Your comment may have breached our community standards. For example it may have been a personal attack, or you might not have used your real name.
Your comment may have been entirely blameless but part of a thread that was removed because another comment had to be removed.
It might have been removed for another editorial reason, for example to avoid repetition or keep the conversation on topic.
For practical reasons we reserve the right to remove any comment and all decisions must be final, but please don’t take it personally.
If you’re playing by the rules it’s unlikely to happen again, so feel free to continue to post new comments and engage in polite and respectful discussion.
For your reference, the removed comment was:
Moderators have removed an entirely rational and reasonable comment by Duncan Mouat. The pattern of deletions is now profuse and appears to be quite consistent in its objection and purpose. Given the repetition and evidently convergent aim of these deletions, can the moderators please provide a clear statement regarding the exact standard(s) these posts are deemed to have offended.
I propose that due respect for your readers and contributors requires nothing less. We should not be left guessing what the editors’ position is on these matters wherein no insult or off-topic commentary has occurred.
Please understand that these deletions resonate especially loudly within a discussion that essentially reflects upon intent censorship.
Over the last 30 to 40 years, an inexorable process has been in train in Melbourne.
A city that once boasted houses with gardens for the majority has given way to the cannibalisation of our gardens in the interests of accommodating an ever-increasing population. Thus, we have seen increasing medium and high density living in our suburbs, with significant and ongoing loss of trees, other vegetation, and space per person. At the same time we have seen encroachments on public land for ever more residential development. To name only two of many examples, there was the Commonwealth Games Village in Royal Park and the Eastern Golf Course in Doncaster, which were both turned into housing developments. The State Government in Victoria now plans to facilitate development on golf courses, according to their definition by a committee of developers as redundant green amenity.
As a result of Melbourne’s increase in population density, our public transport and roads have been struggling to cope for some years. Passengers now only just fit onto trams and trains, level crossings have had to be turned into overpasses and underpasses, in a disruptive and expensive exercise, all over Melbourne. But still the machine which is Melbourne manages to tick along and somehow function. But, to what end? we may ask, as our quality of life steadily diminishes. If Melbourne's inhabitants are just cogs in a big complex machine, built for wealthy international investors in property and finance, then I suppose we have to say it has been a success …until now.
In the last several days a huge number of the "cogs" have had to be de-activated for an indefinite period . The machine can no longer operate as it has been. But the non-essential " cogs" cannot be simply put away in a drawer. This is because they are not actually cogs. They are humans with lives and with needs. The even larger machine of the Australian government is obliged to sustain them all over the country. There is no other way.
The health crisis due to coronavirus must make those in authority and with power question what we have been doing over the last few decades. What has been the aim of the direction that the new economy adopted in the last years of last century? What I have seen is an erosion of our quality of life in many ways, but the loss of land and space per person is the most stark indicator. Now, in the current health crisis that we are virtually locked down in, our living environment, the amenity or lack of it, in our surroundings, is highlighted. How does a person living in a small apartment take care of his or her mental and physical health? This person no longer uses the small apartment simply as somewhere to sleep after returning from work and an evening get together with friends in a public place. This is now "home". Does it pass the test to qualify as such, or is it more like a prison cell?
The corona virus illustrates the great importance of the availability of public space for the population. Yet the public space we now need to practice safe distance in has been greatly reduced by overdevelopment in Melbourne.
Moreover, we cannot always exist as a crowd. We must separate and have our own space. We are individual beings. For those who still have them, private gardens are of huge importance. Their growing rarity is of great significance in Melbourne’s ability to cope with health and social problems. Had the corona virus struck 30 years ago, a far larger proportion of the population would have had such a refuge. Tragically, these gardens have been taken from us, with the push to live more densely. I use the word "push" deliberately" as we have been pushed into it. Planning in Australia’s big cities has amounted to coercion since the 1990s, with loss of formal rights of objection to the massive changes forced upon us.
Many philosophers, cartoonists and commentators have questioned the purpose of our lives - the "rat race", the overcrowding. I am doing the same as this crisis shrieks out for a serious re-evaluation of where we are going. We are barely coping now so how will we cope with 8 million in Melbourne if we have another pandemic?
Covid-19 is a warning. We can take it as such or ignore it if we get through it and come out the other side.
High density, high population, high throughput, globalised manufacturing, global high mobility, are not working for us now. When we first learned in January of the outbreak of Covid -19 in Wuhan my first thought was that "This will be in Melbourne soon." Thirty years ago, I would not have had such a thought because China was so distant and separate. I was right, within a few days it was in Melbourne. On January 25th Australia had its first four cases, the first in Melbourne and another three in Sydney. At this time the city of Wuhan in China was in "lockdown".
I was most alarmed to learn that the disease could be spread by people with no symptoms, and that many did not have symptoms. For me that was the key piece of information that should have dictated government protocol to manage contagion.
By March 2nd, the first two cases of community transmission of Covid -19 were reported in Sydney. One was a woman who caught if from her brother recently returned from Iran and the second was a health care worker, working in close proximity with patients. On March 13th, the Victorian health department announced nine new cases of coronavirus in Victoria, including the state’s first community transmission, and it is now being transmitted at an alarming rate. As at 6.30 p.m. March 28th, Victoria's total case numbers were 685.
Now Victoria is in partial lockdown. We are being asked to stay home as much as possible. Businesses have been closed down, sporting facilities are closed, even beaches are closed in Melbourne. How did our governments let it come to this? If I could see it coming, they should have seen it coming. Why were governments apparently powerless to stop it?
Finally, the Tasmanian Government is now not letting people arrive from the mainland without quarantine. I heard a commentator say that this takes advantage of its geographical status as an island. That’s great, but the rest of Australia is also an island! We have blown our chance to stay clear of this scourge. If we had not blown our chances, people would not have had to die or lose their jobs. To me it is a debacle.
So, people will be spending a lot more time at home. The trouble is that "home" is not what it was thirty years ago. Home is now more likely to be an apartment, rather than a house with a garden. For those with a garden, it is far easier to endure days on end without going outside one's home, than it is for someone in a one-bedroom flat.
Lockdown arrangements have been introduced incrementally, which strikes me as policy on the run, and smacks of "shutting the stable door after the horse has bolted." We hear that schools must remain open and then they are closed. We heard the Prime Minister saying that he is going to a rugby match when most of the people I know had been avoiding crowds for at least a couple of weeks.
Why was a protocol not in place for protecting Australia's population? Now people have died, more will get sick and die, people out of work could lose their houses. The fallout is immense. The only thing I can think of giving the Australian government credit for is being ahead of the even more sluggish World Health Organisation, in declaring Covid-19 a pandemic.
The neo-liberal economy, globalisation, and the pandemic.
The very arrangement that makes money for the few is a bad arrangement for the many. Goods and labour move around the world as though geographical distance were meaningless. The movement of ships spreads environmental pests. The movement of people spreads disease. With the increased population density in Melbourne and other cities, due to rapid population growth, mostly from overseas migration, we in Australia are more likely to have close encounters with strangers than we would have had before Australia’s population numbers were ramped up. On a day like today - sunny and warm in autumn - we crave a walk outside. We think of the beach, but hesitate because others will be thinking the same, and it will be hard to walk on the now defined pathway without encountering people at close quarters, even briefly.
Victorian Senator Sarah Henderson was heard on the ABC a few days ago, saying that she had been a strong proponent of upgrades to the Great Ocean Road but now she urges people not to come to coastal towns even if they own "holiday houses" there. The recent obsession with increased mobility in this state is now something that will only serve Covid -19. Small towns have welcomed the commerce that tourism brings, but now it is unimportant compared with the need to stay isolated.
Australia's ailing economy: Economic stimulation means increasing human transactions and disease transmission
Stimulus packages surely are meant to stimulate the very behaviour that spreads the disease. They contradict moves to save the health of the nation. That is, they aim to increase economic activity, to wit transactions, whilst locking down decreases transactions. The responsibility of the government now is to support the population directly affected by the measures taken to save the health of the population. Those people directly affected are paying a big price.
This plague was forecast
Scientists have warned us for decades that a pandemic was overdue. We even knew it was likely to come from China in the form of a zoonose. We got a real-time warning when we first knew of the deadly virus in Wuhan. Despite all these warnings, we did not act quickly enough and we are now dealing with an exponentially rising number of Covid-19 cases. Our lives have been de-railed. Next time, we need to be ready to pull up the drawbridge sooner. We also need to be prepared in terms of manufactured goods. Supermarkets need to have warehouse supplies. Deliveries "just in time" are inadequate. We need more medical and nursing staff. We cannot just wear our health workers into the ground. Hospital cleaners and hospital management need to be prepared and knowledgeable in disinfection protocols and practices. Government needs to have more of a role in the economic structure of the country, taking health into account as an absolute priority, even if it's not economically rational!
When this crisis has passed will we go back to "Business as Usual," and again flounder just as badly when Covid -21 or 23 arrives?
On 27 March 2020, the AWU and Master Builders Australia jointly called on governments to ensure the continued operation of the building and construction industry, claiming that without it the economic knock-on effects would be devastating on a scale that would dwarf what we have seen to date.
There is no question that many dependencies on this very costly and demanding industry would cause more economic disruption, but what about safety with regard to COVID-19? Although the industry argues that it can be safe, we will argue that the industry is not suited to workers keeping safe distances. On the principle that a stitch in time saves nine, it would be better to shut down sooner rather than later because the later action is taken, the worse the grip of COVID-19 will be on the economy. Since the virus has caused the government to cease the mass migration that has driven huge expansion in the construction industry, demand has dropped, and now is the perfect time to massively curtail construction industry activity. In the meantime, will the industry take responsibility for the return home of the many temporary migrant construction workers from China and Indonesia who, unlike international cruise-ship passengers, are already onshore, virtually invisible, but numerous? And an industry worker argues that the industry is not capable of adapting to safe distance practice.
“The shutdown of the construction industry would jeopardise not just those employed directly, but the whole livelihoods of millions of Australians employed in precarious sectors like manufacturing. It would devastate nationally important industries in the building supply chain, like the $30 billion steel industry,” say the AWU and MBA.
This shows that we have become too dependent on this industry. It has an unhealthy hold on our economy, our political system, our politicians and political parties. This hold has destroyed business, industry and employment diversity in Australia, because agriculture and ordinary manufacturing cannot compete with the inflated profits of the rapidly metastasizing property development sector, which attracts finance away from other sectors.
The same industry has successfully lobbied decades for faster and faster population growth, via mass immigration, to drive demand for its product. Now the demand will dry up as immigration has been stopped, finally providing an interruption to property-development’s hold on our economy.
As well as importing customers, the industry has also exploited many temporary migrants, undermining immigration rules, safety, wages and other employment conditions. The industry may have profited, but prices have risen and standards have dropped, to the extent that buildings over three stories are now uninsurable.
The AWU and MBA argue that, “Forcing the industry’s closure would also blunt the impact of federal, state and territory government stimulus packages as infrastructure projects would immediately grind to a halt. Civil construction, in particular, must continue to build the nation and can do so safely given the nature of its sites.”
The cry of ‘nation-building’ has led to overdevelopment with disastrous drops in building standards and environmental amenity. Australians have suffered from constant upheaval and loss of democracy as government outsourced planning to developers. In the name of catering to unprecedented population growth, Australian cities, suburbs and regions have been taken out of the control of their residents, subjected to constant infrastructure expansion, road-building, traffic diversions, and destruction of loved environment.
The AWU and MBA’s line is: ”Indeed, the catastrophic threat of a construction shutdown means the whole construction industry has a civic duty to impress upon authorities it can operate while ensuring compliance with social distancing and hygiene requirements.”
How could anyone have confidence in an industry known for corrupting government at all levels, bullying, unaccountability, uninsurability, and lawlessness? This industry has seen thousands of Australians bankrupted and homeless. Multiple inquiries into its dysfunctionality have failed to reform it. It is time to stop dancing to the demands of this industry. Australia has been living beyond its means in an artificially and unreasonably accelerated growth period.
The AWU and MBA try to present a picture of reform and responsibility:
“That means everyone in the industry has to step up and be accountable. Construction companies and project managers must ensure that protocols at their site are enforced. Construction workers owe it to each other and their families to be responsible and do the right thing. This is only the only way the industry can continue working while reducing the risk of COVID-19 transmission.”
Unsafe: Safe distance mostly impossible in Construction industry
An industry worker, who prefers to remain anonymous, says:
“Practising safe distance at building sites for most activities is impossible.
It is generally not safe for one person to work alone in the industry. Usually construction sites involve many people in many activities simultaneously, crisscrossing each other in small and often confined spaces, sharing narrow temporary paths and causeways.
In multi-storey building construction, hoists are used to bring people to various floors. These hoists are always crammed with people. It is not affordable to take people (or loads) one at a time.
Concreters work closely together when they lay concrete, frequently in small areas. You might have one worker using a scrider, and two others using a shovel or a vibrator, not even half a meter from each other. You will often get four or five people a couple of meters square, due to the need to act together to carry out the work. It would be hard or impossible for one person to do such work alone. It would be uneconomical for less than four or five.
High-rise work employs huge crowds of skilled and unskilled workers. It is common in the construction of a multi-storey building to have 40 steel-fixers and 40 form-workers operating simultaneously on one floor.
The nature of the industry entails very basic conditions of hygiene and shelter. Disinfection and maintenance of disinfection in such areas, where many workers are coming and going, would require a large-scale dedicated team of cleaners and supervisors with the authority to stop and start work. It would be dangerous to have such teams present on building sites.
Construction sites are scenes of intense activity, with many people interacting on many processes, helping each other. The cost of construction means that things are done as quickly as possible.
When trucks are unloaded, you often have many labourers unloading next to each other.
It is rare for one person to work alone. Generally speaking, in this industry, safety requires workers to work in pairs or in larger groups.
People are often required to work in confined space and they then need another person to assist with tools and equipment, physically handing these from one person to the next.
Transport is often shared. People habitually organise to come and go to work in one vehicle because many jobs are not accessible by public transport.
Many temporary migrants are moved in and out of construction sites in busloads from densely shared accommodation. A large proportion are Chinese and Indonesian. They often do not speak or read any English, and certainly not enough to know how to protect themselves. They tend to be insecure in their employment and visa status and are not likely to exercise their rights to safety, if they know them. These workers are like a separate population on construction sites, with whom only basic communication is possible, usually via their own foreman.
Will the industry now take steps to finance these workers’ return home?”
The AWU and the MBA say in their press release:
”In times of crisis people look to unions, industry, and government to work together. We have to show we can not only slow the spread of COIVID-19 but ensure there's an economy left when the crisis is over.”
The problem is that unions and government have been working for industry and against democracy for too long. Let’s hope the AWU and the MBA, the Property Council of Australia and all the other corporate coercers who have been calling our tune start to adapt to reality for a change.
Last night a nursing home informed me that my 95 year old mother was in isolation, having developed high temperatures. She had been swabbed for COVID-19 and results might be available in two to five days.
I was not at all surprised, not just because of the known vulnerability of patients in nursing homes, but because of my personal experience in nursing and with this nursing home.
A few weeks ago, when COVID-19 was already around, I was asked by staff to come to the nursing home in order to sign a document on behalf of my mother. Anticipating a state of policy paralysis regarding infection control and COVID-19, I wore my own gloves to the nursing home and waited for staff to bring the documents to my car. I produced my own pen to sign with. I noted that the keypad at the entrance of the nursing home was an obvious fomite or transmission source for infection. The nursing staff told me that they had not thought of this. It seemed to me that the only way people might prevent infection via keypad from the hundreds of fingers that touched it each day would be to wear gloves or otherwise place a disposable transparent plastic barrier over it, to be changed for each patient.
My mother is 95 and sustained acute severe brain injury in 2012, with her condition slowly deteriorating further due to failure to treat the causes. She now recognises no relatives or friends. The nursing home has now banned visitors and, in any case, I could not visit her without endangering myself and others, so I have resigned myself to her dying without me, her last close relative. She will be in the presence of various nurses, however, to whom she relates, and who relate to her. It is possible, however, that she will not die, just as it is possible that she does not have COVID-19.
In the meantime I have been in retreat for a couple of weeks to Lake Eucumbene in the high country of NSW, unable to access the internet. I am in company of a very old friend, who belongs to a cohort vulnerable to COVID-19. Will this be the last goodbye, I wonder.
A few days ago we were healthy enough to walk the 16km from Charlotte Pass to Mt Kosiusko peak. A lot of other people seemed to have had the same idea though, although most seemed keen to stay out of each other's way.
This unpaved road where we have taken a villa, has few houses, widely separated, used only for holidays. In the past few days all of them have become inhabited by refugees fleeing virus-infested Sydney.
Although there is substantial mature forest here, there is almost no wildlife, although it is usually teeming. We have seen the same wallaby twice, three brush-tailed possums, one currawong, two kookaburras, a couple of rosellas, and two currawongs. Fires nearby will have destroyed a lot of habitat and inhabitants, but we wonder if the extreme heat in the new year killed most creatures here.
Unfortunately we cannot stay here for much longer. In a week or two I must return to Melbourne, where I maintained a relatively isolated state for several weeks prior. My friend will avoid going home to his flat in Sydney because his family there is exposed to multiple infective sources. He has decided to go and stay in another flat in Sydney that belongs to another friend who is currently stranded in Italy - in the viral epicentre.
Many sad goodbyes in store for so many people in this country as those of us who can, bunk down.
Stay safe at home!
Chloroquine (and hydroxycloroquine) are related drugs that have been used for over 70 years to treat and prevent malaria. They have both antiviral and anti-inflammatory properties.
French studies
Professor Didier Raoult, who has a laboratory and hospital beds in Marseille, France, has been promoting chloroquine as an effective treatment for COVID-19 Coronavirus. From 16 March 2020 he trialed treatment of 24 COVID-19 patients with 600 mg of Chloroquine daily for 10 days.
He reported that six days later only 25% of these patients still carried the virus, whereas without chloroquine one would expect 90% to still be infected and infectious. The implication is that Chloroquin shortened the course of the illness.
The study may also have suggested that additional treatment with the antibiotic azithromycin led to better outcomes where secondary pneumonias of bacterial origin occurred.
Raoult has the qualifications to make serious claims in this field. He is a microbiologist specialising in infectious diseases and a professor in the Medical Faculty at the University of Aix-Marseilles. He is widely recognised for his work. Since 2008 he has been director of the URMITE Research Unit in infectious and tropical diseases.
Although the data are not yet published, the French Government is trying to reproduce the study.
Olivier Veran, Minister for the French government has authorised the use of Chloroquine for treatment of very serious cases of COVID-19, under supervision by hospital medical teams, but does not authorise it for less serious ones. He has said that the French Government is working closely with Raoult's team.
Didier Raoult disagrees with the French Government and says Chloroquine should be used at the earliest stages in the COVID-19 illness.
The French Government is currently carrying out its own formal testing of this treatment, possibly in Lille, according to a report on 23 March 2020, on RT France, https://francais.rt.com/en-ce-moment/72699-chloroquin.
The Chinese Government has used Chloroquine with COVID-19 cases. A Chinese study involving more than 100 patients was described in a letter published in BioScience Trends on 19 February 2020. Researchers said that Chloroquine phosphate was the most effective treatment available to contain the development of the viral form of pneumonia associated with COVID-19, improving the state of the lungs, to shorten the duration of the illness and the presence of the viral infection itself. Apparently the letter has not yet been followed up with formal data from the study.
Anecdotally, Chinese researchers have apparently encountered obstacles in conducting formal trials involving controls because patients have obtained their own drugs in preference to submitting to the uncertainty of being part of a control group rather than a group actually receiving the drug in question.
United States
President Trump has initiated a trial in the United States, following an interview on Tucker Carlson Tonight with a person reporting on Didier Raoult's claims.
Alert observers will, however, notice that Anglosphere reporting on this matter is political, rather than informative. This distraction from essential information for the public complements a race by pharmaceutical companies to corner the US and international market with an expensive 'cure'.
Nonetheless Chloroquine can be used by any doctor to treat anything they consider appropriate in the United States and elsewhere.
The World Health Organisation has also initiated trials of a few drugs, including Chloroquine.
Other countries use of Chloroquine for COVID-19
South Korea reputedly has guidelines that recommend Chloroquine for cases of COVID-19 that require anti-viral intervention and for the elderly. It also recognises its use as a prophylactic against the virus.[1]
In the meantime a number of countries are already using Chloroquine in treatment of COVID-19 with less restrictions.
The Bolivian Republic has begun giving oral Chloroquine to COVID-19 patients and also to their immediate contacts, which tend to involve around 15 people on average, as well as to health professionals working with COVID-19 patients. In Venezuela similar regimes are being undertaken. Algeria
strong> is also using chloroquin for COVID-19 patients.
Use of Tolicizumab in Naples for COVID-19
In Naples there have been trials involving small numbers of hospitalised patients, using another old drug, usually used for arthritis, called Tolicizumab (also sold as Actemra). See "Coronavirus, Napoli: 5 pazienti gravi su 10 migliorano, grazie al Tolicizumab, il farmaco anti artritie." (15 March 2020, Ildenaro.it). The information I was able to access about this trial was fairly old.
This monoclonal antibody used for the treatment of rhematoid arthirits is also effective against COVID-19 pneumonia, claim doctors involved in its use in Naples. This treatment was inititiated in Naples by Paolo Ascierto, Director for the Pascale Immunological Clinic and Vincenzo Montesarchio, infection specialist at Cotugno Hospital in Naples.
For Saturday 7 March the two doctors said that ten patients, of whom 7 were intubated [presumably for pneumonia] and three had respiratory difficulty [but were unintubated], experienced strong improvement compared to controls. The first patient treated had improved enought to have his intubation removed. Of the other patients, four stabilised and one, unfortunately, quickly died from respiratory distress. Of the other three patients who where not intubated, after about 24 hours one was stable and one had shown signs of clinical improvement.
The doctors also said they had received optimistic signs from other centres: Treatment centres or hospitals in Fano/Pesaro reported improvement in eight patients treated in a total of eleven. And a Dr Chiari from United Hospital in Padova South reported improvements in two patients treated over the previous 24 hours.
NOTES
My reference for this is called "An Effective Treatment for Coronavirus (Covid-19)," a paper attached to "Fosfato di Clorochina e Coronavirus," https://youtu.be/8TpvDixTivw., a presentation by James M. Todaro, MD Columbia and Gregory J. Rigano, Esq.. It was initially published as, "in consultation with researchers at the Stanford University School of Medicine, the UAB School of Medicine and the National Academy of Sciences, March 13, 2020." Stanford Univ has distanced itself. It looks as if the writers may have discussed things informally with various university researchers who did not expect to be named and quoted. [Good luck finding the article because at the moment the author is reduced to using a brand-name mobile phone that makes it almost impossible to see the URLs for articles.]
TAGS: coronavirus, COVID-19, Didier Raoul, France, international, Trump, controversy
Countries like the US, England, France, Spain and Germany are about 9-10 days behind in the COVID-19 progression. For our benefit, the video channel called "A THING BY" asked Italians to record a message they wish had heard 10 days prior. Let's take careful note of what they have to say.
Our version of capitalism is something the narcissistic writer Ayn Rand would have adored, but in a headlong rush to hyper-individualism, have we chosen freedom of the individual over the survival of our species…
Host Ross Ashcroft is joined by economist and author, Professor Steve Keen to discuss why coronavirus has closed capitalism.
Cardiologist, Professor Jepson, urges people with cardiovascular risk issues to take more control of their situation.
Getting to the heart of Covid-19
Advice for Australians with heart risk factors in evolving situation, from Professor Nigel Jepson, medical director of Eastern Heart Clinic, Randwick, NSW. Professor Jepson's summary is:
· That Australia [...] ‘must increase vigilance and adopt even stricter measures’ to avoid the trajectory [that COVID-19] has taken in Northern Italy,’ says Professor Nigel Jepson, interventional cardiologist at Prince of Wales Hospital and Medical Director of Eastern Heart Clinic, Randwick NSW.
· Particularly vulnerable are the 1.2 million Australians currently living with cardiovascular disease (CVD);[1] more than 1 in 4 (26%) of those aged 75 and over have heart, stroke and vascular disease.[2]2
· This group and people with other conditions that affect the heart and vascular system, such as high blood pressure, chronic respiratory disease and diabetes, are at elevated risk of developing complications if they contract COVID-19.3 In an ordinary year, CVD already leads to an average of more than 1 million hospitalisations.2
· In addition to following the Government’s advice on social distancing and hygiene, Prof Jepson advises that people with CVD should start following ‘heightened’ measures(below).
· ‘We can see from the data in Wuhan that patients with an underlying heart condition may not be more likely to become infected in the first place but are at higher risk of developing complications including breathing problems, abnormal heart rhythms or, ultimately, heart failure, than others,’ says Prof Jepson. This increased risk of death for people with CVD is estimated to be nearly 10% higher than a ‘healthy’ patient.[3]
· ‘We don’t want to create fear or panic but I don’t think we’re really getting the message across that, while for most of us COVID-19 would be an innocuous disease to get, we need to adopt caution and care to slow the rate of spread as much as possible, in order to protect those who could be more seriously affected.
· ‘We also want to avoid clogging up hospitals. It makes no sense to say, ‘Let’s all get it now, and get it over with’ - that’s nonsensical and dangerous - because we need the emergency beds, equipment and personnel for acute COVID-19 patients or any other person requiring emergency medical care, or we will find ourselves buckling under the pressure, like the health services in Lombardy (northern Italy)’.
· New Italian data released at the weekend shows higher death rates than in China, Iran or Korea.[4] The precise reasons for the higher rates are not clear, but it is thought that very rapid community spread of COVID-19 and a saturated health system were at least significant contributors.
10 WAYS PEOPLE WITH HEART ISSUES CAN REDUCE THEIR COVID-19 RISK:
1. Avoid large gatherings (even contexts with fewer than 500 people) e.g theatres, cinemas, concerts and shopping centres [Candobetter Editor says, Oh, come on, Prof Jepson, stop the pussyfooting, surely you mean much smaller crowds, to wit, avoid groups.]
2. Exercise caution when using public transport - avoid busy times and routes in known outbreak areas; make alternative travel arrangements
3. Do not travel unnecessarily - avoid airports, train stations and bus terminals
4. Go shopping at quiet times- or take advantage of major supermarkets’ time slots for older people only
5. Have your prescriptions for heart medicines filled now – ask your pharmacist and GP to assist as shortages are occurring in some areas
6. Postpone non-urgent medical appointments or procedures - or consult your healthcare professional by phone or ‘telehealth’ instead
7. Stock up on groceries (within reason) – you’re going to be at home more, so organise for online deliveries (friends and family can help)
8. Get vaccinated – stick to plans to be vaccinated for influenza and pneumonia, and others as your doctor advises, to avoid developing other conditions that can be confused with coronavirus (such as flu)
9. Stay healthy - eat well, get enough sleep and follow exercise regimens as advised by your healthcare professionals
10. Keep calm and carry on - if you live alone, think about low-risk activities you can do to socialise, such as meeting a friend outdoors for a walk
Professor Nigel Jepson is the medical director of Eastern Heart Clinic, one of the largest interventional cardiology hospitals in Australia, based at the Prince of Wales Hospital at Randwick. He is also a senior staff cardiologist at the Prince of Wales Hospital, where he established the unit’s trans-catheter aortic valve program.
3. Chinese Center for Disease Control and Prevention, CCDC Weekly, Vol 2, No. 8
4. World Health Organisation Situation Reports 16 March 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200316-sitrep-56-covid-19.pdf?sfvrsn=9fda7db2_2
 RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come.
RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come. The Royal Australian College of General Practitioners (RACGP) is warning government that GPs will need adequate resources to manage the long-term care of COVID-19 positive patients. The RACGP has released a guide for GPs providing care to adult patients who have previously tested positive to COVID-19 or have a history suggestive of undiagnosed COVID-19 and have - or are at risk of - post-COVID-19 conditions. The guide was developed in collaboration with HealthPathways. RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come.
The Royal Australian College of General Practitioners (RACGP) is warning government that GPs will need adequate resources to manage the long-term care of COVID-19 positive patients. The RACGP has released a guide for GPs providing care to adult patients who have previously tested positive to COVID-19 or have a history suggestive of undiagnosed COVID-19 and have - or are at risk of - post-COVID-19 conditions. The guide was developed in collaboration with HealthPathways. RACGP Acting President Associate Professor Ayman Shenouda said that GPs would be managing the long-term impacts of the virus on some patients for years to come. [English translation of video-dialogue below the video.] In this very interesting video, Frederic Taddei of Interdit d'interdire (Forbidden to censure) states, at the beginning, that he has no intention of evaluating the value of hydroxycloroquine and azithromycine, because he lacks the medical knowledge to do so. He states his intention in inviting his guests (Olivier Berruyer, economist and statistician, and Raphaël Liogier, sociologist and philosopher) is to find out why there is so much controversy over Professor Didier Raoult and his promotion of COVID-19 treatment using hydroxychloroquine. [Note that this unpolished translation took hours out of several days. Both debaters spoke emotionally and with multiple redundancies, also different versions of the word hydroxychloroquine.] Among other things, the participants' discussion of the politics seemed to boil down to the ambiguity of testing drugs in a pandemic situation where big-pharma, other commercial competition, and fraud, loom. I thought that the main argument could be summarized as: (Olivier Berruyer) 'The effectiveness claimed by Didier Raoult for hydroxychloroquine could only be proven through randomised double-blind trials, but these have never been successfully completed due to a series of mishaps', and 'There is no way anyone could scientifically reproduce Raoult's method because he keeps changing it', versus (Raphael Liogier) 'Pending a perfect cure for COVID-19, Didier Raoult is doing the best he can as he treats people in a personalised manner, monitoring their responses, with drugs he believes to be effective'. I would add that, as the translator, and as an evolutionary sociologist, my own feeling about the reasons for such controversy is that it is related to the way apes behave over a tasty food supply or some other big event (good or bad) that concerns them. It is natural for everyone in the community to get involved in something important - in this case a pandemic. We seize whatever handle, whatever fact or factoid we can get hold of, and we run with it, to the best of our ability and enthusiasm. Apes with alpha-pretensions get up in trees and shout loudly about what they've got, competing for audiences and power. So, I invite the reader to keep in mind ape-ethology when he/she reads the translated dialogue below. {See also the notes at the end, on hyrdoxychloroquine trials and prescription of this drug and the law in France.)
[English translation of video-dialogue below the video.] In this very interesting video, Frederic Taddei of Interdit d'interdire (Forbidden to censure) states, at the beginning, that he has no intention of evaluating the value of hydroxycloroquine and azithromycine, because he lacks the medical knowledge to do so. He states his intention in inviting his guests (Olivier Berruyer, economist and statistician, and Raphaël Liogier, sociologist and philosopher) is to find out why there is so much controversy over Professor Didier Raoult and his promotion of COVID-19 treatment using hydroxychloroquine. [Note that this unpolished translation took hours out of several days. Both debaters spoke emotionally and with multiple redundancies, also different versions of the word hydroxychloroquine.] Among other things, the participants' discussion of the politics seemed to boil down to the ambiguity of testing drugs in a pandemic situation where big-pharma, other commercial competition, and fraud, loom. I thought that the main argument could be summarized as: (Olivier Berruyer) 'The effectiveness claimed by Didier Raoult for hydroxychloroquine could only be proven through randomised double-blind trials, but these have never been successfully completed due to a series of mishaps', and 'There is no way anyone could scientifically reproduce Raoult's method because he keeps changing it', versus (Raphael Liogier) 'Pending a perfect cure for COVID-19, Didier Raoult is doing the best he can as he treats people in a personalised manner, monitoring their responses, with drugs he believes to be effective'. I would add that, as the translator, and as an evolutionary sociologist, my own feeling about the reasons for such controversy is that it is related to the way apes behave over a tasty food supply or some other big event (good or bad) that concerns them. It is natural for everyone in the community to get involved in something important - in this case a pandemic. We seize whatever handle, whatever fact or factoid we can get hold of, and we run with it, to the best of our ability and enthusiasm. Apes with alpha-pretensions get up in trees and shout loudly about what they've got, competing for audiences and power. So, I invite the reader to keep in mind ape-ethology when he/she reads the translated dialogue below. {See also the notes at the end, on hyrdoxychloroquine trials and prescription of this drug and the law in France.)
 With COVID-19, we should not just be looking at deaths. Deaths may actually be a poor indicator of the damage this virus may do. We should be looking at a continuum, as in: If the proportion of people who contract COVID-19, and who are over 80, die, what happens to those (of any age) who live? Given the ability of this disease (unlike flu) to cause clotting problems all over the body, affecting organs which affect other organs, we should be expecting that a proportion of survivors will have various rates of blood clots and organ damage. What proportion of these will clear, improve, or become chronic and dangerous? How long will how many survivors survive? Check out the following videos by doctors regarding clotting and organ-damage.
With COVID-19, we should not just be looking at deaths. Deaths may actually be a poor indicator of the damage this virus may do. We should be looking at a continuum, as in: If the proportion of people who contract COVID-19, and who are over 80, die, what happens to those (of any age) who live? Given the ability of this disease (unlike flu) to cause clotting problems all over the body, affecting organs which affect other organs, we should be expecting that a proportion of survivors will have various rates of blood clots and organ damage. What proportion of these will clear, improve, or become chronic and dangerous? How long will how many survivors survive? Check out the following videos by doctors regarding clotting and organ-damage.  Ivor Cummins is a health writer and biochemical engineer, who calls himself The Fat Emperor. He has drafted
Ivor Cummins is a health writer and biochemical engineer, who calls himself The Fat Emperor. He has drafted  Innes Willox, the Chief Executive of the Australian Industry Group or
Innes Willox, the Chief Executive of the Australian Industry Group or  The extension of State of Emergency in the other five states does not need legislation, unlike Victoria. Here's information on the relevant laws for comparison, plus actions taken under similar legislation for COVID-19 in states outside Victoria. We have also now received a
The extension of State of Emergency in the other five states does not need legislation, unlike Victoria. Here's information on the relevant laws for comparison, plus actions taken under similar legislation for COVID-19 in states outside Victoria. We have also now received a 
 The girls needed a break. The university term had just finished and so had "lock-down". Students, Isla and her two housemates, Chloe and Emily, were anxious to escape Melbourne. Emily's friend Olivia who was studying at Adelaide University had been trying, for more than a year, to entice Emily over for a visit, and this seemed the opportunity. Of course all three girls would go over together and, as they all yearned for a seaside experience, after spending so much time in their rented inner suburban house, they booked into an apartment for five nights in Glenelg, not far from Emily. It would be great! They could go for walks along the beach every morning!
The girls needed a break. The university term had just finished and so had "lock-down". Students, Isla and her two housemates, Chloe and Emily, were anxious to escape Melbourne. Emily's friend Olivia who was studying at Adelaide University had been trying, for more than a year, to entice Emily over for a visit, and this seemed the opportunity. Of course all three girls would go over together and, as they all yearned for a seaside experience, after spending so much time in their rented inner suburban house, they booked into an apartment for five nights in Glenelg, not far from Emily. It would be great! They could go for walks along the beach every morning!



 It was a stifling summer night with the usual crowd at the jazz venue Jonathan had frequented regularly for the previous few years. On this particular night he was introduced to Ruth, a rather earnest, slim, dark haired lady, in her early thirties. Jonathan, although somewhat lonely following the recent acrimonious break-up of his marriage to Danielle, and consequent distancing from his young son David, was not seeking a new partner. He felt the need to sort out his feelings and his finances before taking steps in that direction. He and Danielle had sold the family home in North Caulfield, and now he had to find another house with only half the funds, while house prices were sky-rocketing. He really needed to get away by himself to think about his future.
It was a stifling summer night with the usual crowd at the jazz venue Jonathan had frequented regularly for the previous few years. On this particular night he was introduced to Ruth, a rather earnest, slim, dark haired lady, in her early thirties. Jonathan, although somewhat lonely following the recent acrimonious break-up of his marriage to Danielle, and consequent distancing from his young son David, was not seeking a new partner. He felt the need to sort out his feelings and his finances before taking steps in that direction. He and Danielle had sold the family home in North Caulfield, and now he had to find another house with only half the funds, while house prices were sky-rocketing. He really needed to get away by himself to think about his future.
 Early this year, as the COVID-19 virus gained a toehold in Australia, the message from governments, via the media, was that the aim was to "flatten the curve" so that case numbers would be such that our hospital systems would not be overwhelmed. It was not to eliminate the virus altogether.
Early this year, as the COVID-19 virus gained a toehold in Australia, the message from governments, via the media, was that the aim was to "flatten the curve" so that case numbers would be such that our hospital systems would not be overwhelmed. It was not to eliminate the virus altogether. 
 In Melbourne last Saturday nine public housing towers with 3,000 residents were shut down for at least five days, due to a large cluster of identified cases of COVID-19 within their walls. Since then, of course, the whole of Melbourne has been locked down for about six weeks. And this is a Melbourne burgeoning with high-rises. It seems a lifetime ago, but it is only about five months since the cruise ship, Diamond Princess, with identified cases of COVID-19 was unable to disembark in Yokohama, Japan. Her hapless passengers were confined to their cabins, in an attempt to prevent the spread of the virus aboard the ship and on land. Predictably however, the virus spread through the ship and by early March there were six casualties.
In Melbourne last Saturday nine public housing towers with 3,000 residents were shut down for at least five days, due to a large cluster of identified cases of COVID-19 within their walls. Since then, of course, the whole of Melbourne has been locked down for about six weeks. And this is a Melbourne burgeoning with high-rises. It seems a lifetime ago, but it is only about five months since the cruise ship, Diamond Princess, with identified cases of COVID-19 was unable to disembark in Yokohama, Japan. Her hapless passengers were confined to their cabins, in an attempt to prevent the spread of the virus aboard the ship and on land. Predictably however, the virus spread through the ship and by early March there were six casualties.
 Daniel Ziffer's journalistic effort for the ABC Saturday May 9th,
Daniel Ziffer's journalistic effort for the ABC Saturday May 9th, 

 Will governments buy back vital resources and essential services from the embattled private sector, or will they allow the wealthy to pick up resources and monopolies cheaply, pressing the unemployed and endebted into slave-like conditions? Can we adapt to or avoid a future that appears to hold more and worse pandemics? If COVID-19 is a pandemic designed for elite purposes to cull the aged and weak, why have some governments tried to protect their vulnerable populations? We have obviously become too economically dependent on the model of continuous accelerated growth in human numbers and human activities globally to be able to protect ourselves from the pandemics that come with this economic model. At the same time the long-predicted oil-resources breakdown in supply is looming. Can any good come of this? Is this an opportunity?
Will governments buy back vital resources and essential services from the embattled private sector, or will they allow the wealthy to pick up resources and monopolies cheaply, pressing the unemployed and endebted into slave-like conditions? Can we adapt to or avoid a future that appears to hold more and worse pandemics? If COVID-19 is a pandemic designed for elite purposes to cull the aged and weak, why have some governments tried to protect their vulnerable populations? We have obviously become too economically dependent on the model of continuous accelerated growth in human numbers and human activities globally to be able to protect ourselves from the pandemics that come with this economic model. At the same time the long-predicted oil-resources breakdown in supply is looming. Can any good come of this? Is this an opportunity? 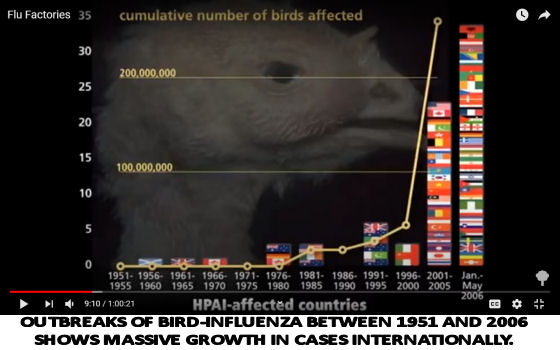
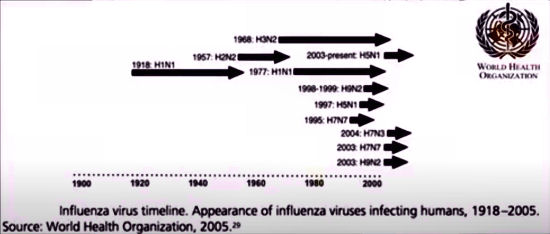
 In this article, Sally Pepper proposes that there is an economy with a small 'e' and The Economy with a big 'E'. As well as threatening its survival, COVID-19 has called the big E economy into question. Sally says, "The economy with a small 'e’ is a way of describing what we do. The Economy with a capital “E” is something we serve, whether we like it or not. To please The Economy we have to behave in such a way that it looks its best and is pleased with itself. The Economy seems to be like a teenage boy, with a voracious appetite. It never develops beyond the need to grow bigger, endlessly. It is like a monster that we have given rise to and are doomed to cater to forever."
In this article, Sally Pepper proposes that there is an economy with a small 'e' and The Economy with a big 'E'. As well as threatening its survival, COVID-19 has called the big E economy into question. Sally says, "The economy with a small 'e’ is a way of describing what we do. The Economy with a capital “E” is something we serve, whether we like it or not. To please The Economy we have to behave in such a way that it looks its best and is pleased with itself. The Economy seems to be like a teenage boy, with a voracious appetite. It never develops beyond the need to grow bigger, endlessly. It is like a monster that we have given rise to and are doomed to cater to forever."
 Dear Censorial Overseers
Dear Censorial Overseers
 On 27 March 2020, the AWU and Master Builders Australia jointly called on governments to ensure the continued operation of the building and construction industry, claiming that without it the economic knock-on effects would be devastating on a scale that would dwarf what we have seen to date.
On 27 March 2020, the AWU and Master Builders Australia jointly called on governments to ensure the continued operation of the building and construction industry, claiming that without it the economic knock-on effects would be devastating on a scale that would dwarf what we have seen to date. Cardiologist, Professor Jepson, urges people with cardiovascular risk issues to take more control of their situation.
Cardiologist, Professor Jepson, urges people with cardiovascular risk issues to take more control of their situation.
Recent comments